HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights – including our new podcast – puts the vast depth of HMA’s expertise at your fingertips, helping you stay informed about the latest healthcare trends and topics. Below, you can easily search based on your topic of interest to find useful information from our podcast, blogs, webinars, case studies, reports and more.
Healthcare executives gathered with HMA leaders in March to learn and share about new initiatives in quality improvement. Panels and discussions were led by esteemed experts, who provided important insight into the multitude of opportunities to improve quality and equity:
From the Experts: CMS has doubled down on its commitment to improve healthcare quality, equity, and access.
The HMA Point of View: Current leadership in Washington has set very clear goals to improve health equity, aligning federal policy as a lever to improve healthcare outcomes. Federal dollars passed along to states are including new rules and objectives to improve quality in an equitable manner. Therefore, those applying for federal contracts and grants must include a strategy to improve quality, equity, affordability, and access.
From the Experts: Interventions need to be robustly evaluated to address equity and social determinants of health (SDOH).
The HMA Point of View: Governments, care providers, and payers have been experimenting with approaches to SDOH, but the bar is now higher and results have to be measurable. New investments that address SDOH and aim to improve equity must include a strategy to measure and analyze results of interventions, including evaluation of critical subpopulations to address disparities. Although experiments will continue, we have reached the point where a robust analysis of outcomes is an expectation.
From the Experts: Quality is playing a central role in operationalizing equity.
The HMA Point of View: While there are many reasons for disparities in health, quality metrics and programs must be designed to improve quality for all patients. Identifying inequities is only the first step; successful programs will advance equity by reducing barriers to care. Measurable quality programs should be designed for population health, but personalized for individuals with clear provider incentives to not only identify disparities but also minimize them. Quality is the tool by which we achieve health equity.
From the Experts: We are on the precipice of doing great things in quality.
The HMA Point of View: Our ability to integrate data from multiple sources is finally getting to a place where patients can get the quality care they need, and providers can give the right care at the right time to improve outcomes. Policymakers have broken down barriers to data sharing, enabling a new economy of information sharing that promises to empower patients and reduce costs. It is no longer enough to have a separate IT or data strategy; anyone working to improve healthcare quality needs to have data strategies within and across every operational function across their organization.
From the Experts: Being rewarded for doing what’s right for the patient is central to continuous quality improvement.
The HMA Point of View: Quality care for the patient means creating the right incentives for payment and care delivery that focus on outcomes and experience. Every point of care in the patient’s health journey needs to be evaluated and designed from the point of view of providing a quality experience. Not every patient has the same journey, and our healthcare system must meet them where they are, delivering for their unique needs. Convenience, personalization, accuracy, simplification, and affordability are nearly as important as clinical outcomes in the mind of most patients and addressing barriers to health can have clinical benefits.
HMA has a long history of working with clients to achieve their quality improvement goals including securing accreditation for both payer and provider organizations, driving clinical practice transformation, and improving the overall value of care. We strongly believe that there is no quality without equity, access, and measurement, and are investing in people and resources to support these needs. Together we are working with clients to advance value-based care, develop programs demonstrating quality, value, and equity in behavioral health, and implement new quality and accreditation programs to better serve their communities.
Learn more about HMA’s continuing work in quality and accreditation and join the conversation on LinkedIn and Twitter using #HMAtalksQuality.
This week’s In Focus is the second in a two-part look at the Centers for Medicare & Medicaid Services’ (CMS’s) recently proposed changes to the Medicaid program. Last week we covered CMS’s proposed changes to the federal Medicaid managed care regulations (CMS-2439-P). This week we review the Medicaid Access to Care proposed rule (CMS-2442-P).
As we discussed last week, the managed care and access to care rules include significant changes to core structural and financing aspects of the Medicaid program. Though state agencies, providers, health plans, consumer groups, and other stakeholders will want to understand the distinct requirements and expectations in each rule that apply to them, the proposed changes cannot be viewed in isolation.
The Access to Care rule addresses a range of challenges that shape the experience of Medicaid enrollees, regardless of whether they are in managed care programs or traditional fee-for-service (FFS). The proposed policy changes also are designed to create an updated federal framework for Medicaid’s home and community-based services (HCBS) programs. These proposals come at a pivotal time, as states are facing workforce shortages, particularly among HCBS direct care workers (DCWs).
The remainder of this In Focus delves into notable components of the proposed changes and includes analysis of the implications of these policies for stakeholders. CMS will benefit from stakeholder input; the deadline for submitting comments is July 3, 2023.
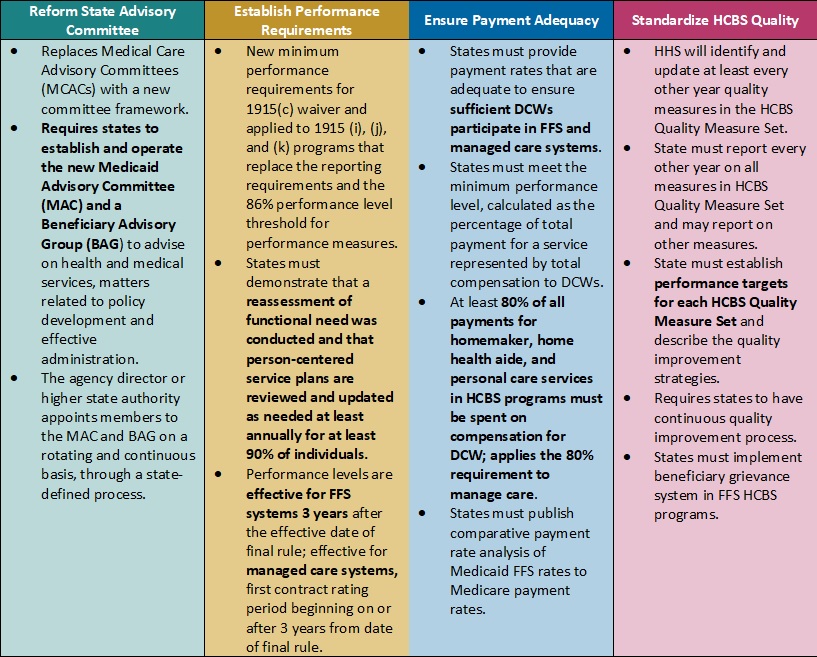
Table 1. Access to Care Regulations: Overview of Proposed Changes
Key Themes and Considerations
Ensuring Payment Adequacy for Key HCBS Services Experiencing Workforce Shortages. One of the most notable proposed changes that would directly impact DCWs is a requirement that at least 80 percent of Medicaid payments be spent on compensation. The proposed rule would apply to homemaker, home health aide, and personal care services, as they represent a large portion of HCBS services that DCWs provide. The proposal is based on feedback from states that have implemented similar provisions, which have ranged from 75 to 90 percent compensation requirements.
CMS specifically seeks stakeholder feedback on the percentage that should be adopted. This policy provision also is important from an equity perspective, given that 90 percent of DCWs are women and 60 percent are members of racial or ethnic minority populations. However, increased or mandated DCW rates may make it difficult for HCBS providers to sustain their businesses as they manage the increased administrative pressures of electronic visit verification, the complexity of filing claims for managed long-term services and supports (MLTSS), and the additional work that HCBS quality measurement may create. Smaller HCBS providers, some of which may have deep cultural expertise, may struggle to sustain themselves and meet these requirements.
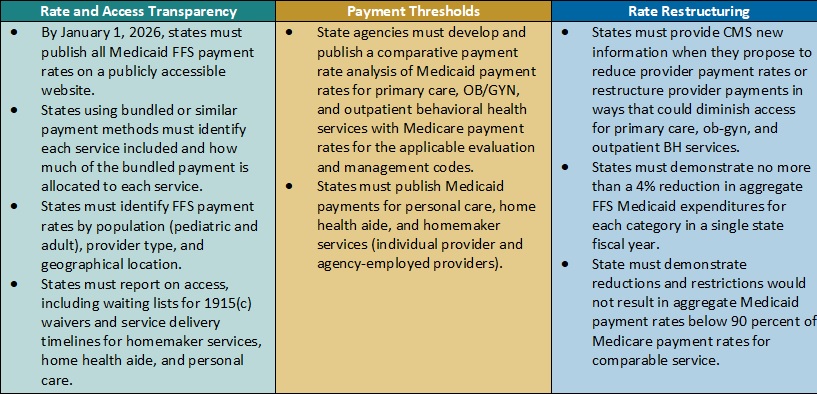
Table 2. Access to Care Regulations: Snapshot of Proposed Rate, Access, and Payment Changes
Payment Alignment. CMS is seeking to align access to care strategies and payment rate transparency more closely across the FFS and managed care delivery systems. The proposed rule includes several changes that CMS has developed achieve this goal. For example:
CMS plans to require that states publish more detailed rate information in a consistent format. States, health plans, providers, and other interested stakeholders will want to consider the implications by delivery system. Additional transparency requirements could create a new opportunity to understand rates across payers and states and use this information in addressing access challenges for services.
The proposed rule also would require extensive comparative analysis of Medicaid FFS rates and Medicare rates. CMS proposes to use Medicare non-facility payment rates as a benchmark to determine if states are meeting federal Medicaid access State analyses will be vital to CMS oversight as well as advocacy efforts within states to monitor and update FFS rates as needed.
Strengthening the Focus on Quality in State HCBS Programs. Over the last several decades, states and Medicaid stakeholders have made significant progress toward increasing participation in HCBS programs and community integration initiatives to counter Medicaid’s institutional bias. CMS is proposing more consistency in the expectations and reporting for HCBS quality measures to further the impact and create a consistent foundation for the recently mandated HCBS quality initiatives starting to take root.
In the short-term, the proposed changes will require states, and likely downstream providers and Medicaid agencies, to immediately change their quality reporting policies and systems. States and their stakeholders will want to map out processes for cyclical updates to HCBS quality measures, including cross-walking the future measures with existing ones, making systems changes, and updating dashboards. Targeted attention and focus will be needed to identify realistic HCBS performance targets that yield successful improvement strategies in the midst of a workforce crisis. Longer term, it will be necessary to map out when updates and reporting will be required to strengthen the rigor and accountability for state performance in the HCBS quality measure set, as well as reinforce the information available to make policy, clinical, and operational improvements to Medicaid programs.
HCBS Access Measurement. CMS is proposing new FFS HCBS payment and access transparency requirements to ensure compliance with Medicaid provider payment rules that require payments to be adequate to enlist at least the same number of providers that the overall geographic population can access. Because the targeted HCBS services do not have a comparable Medicare rate, CMS proposes implementation of a payment rate disclosure approach that would standardize data and monitoring across service delivery systems, with the goal of improving access. In addition to proposed payment transparency changes, CMS proposed new reporting on HCBS waiver waiting lists and timelines for the start of related services once authorized.
These new reporting requirements will provide stakeholders with more information to benchmark their state’s experience with other providers across the nation. This information could be influential to policymakers and legislators and help uncover some of the core contributors to our nation’s HCBS workforce shortage.
Improving Health Equity with Medicaid Beneficiary Input. CMS proposes overhauling the scope and membership of the state Medical Care Advisory Committee. The new Medicaid Advisory Committee (MAC) would continue to advise the state on health and medical matters and play an expanded advisory role on matters of policy development and effective administration of the program. CMS also plans to require that states establish a Beneficiary Advisory Group (BAG) composed of current or past Medicaid beneficiaries. A subset of BAG members would serve on the MAC to ensure their perspectives are integrated into the committee’s recommendations to states.
Under the new federal requirements, MAC representatives could have greater relative input and influence on policies and actions each state Medicaid agency advances. Medicaid stakeholders will want to ensure the MAC’s minimum federal requirements support effective structures and processes in states.
What’s Next
CMS plans to reframe Medicaid access as one of three parts of the continuum of care, along with enrollment and maintenance of coverage. The proposals in the Access to Care rule would have a meaningful impact on the volume and type of data available to evaluate the relationship between Medicaid payment rates and access across all delivery systems.
States, managed care organizations, providers, Medicaid enrollee advocacy organizations, and other interested stakeholders should analyze the proposals and consider submitting comments to CMS on the feasibility, potential impact, and, where applicable, alternatives to the proposed changes. They also can use this time to begin planning and determine which resources and tools they may need to prepare for implementation of changes across delivery systems in the Medicaid program.
HMA’s experts are taking a wholistic approach to reviewing the Access to Care and Managed Care proposed rules in tandem and identifying key points of intersection.
For more information on the access to care proposed rule, contact our experts below.
Policy crossroads and the end of the public health emergency due to COVID-19
This is part of a three-part series on significant implications of the end of the Public Health Emergency (PHE).
The end of the Public Health Emergency on May 11, 2023 is likely to mark a transitional point in the rapidly evolving arena of virtual care services and not a dramatic end of coverage. Coverage of virtual care services will continue to evolve significantly over the next five years given the exponential growth in the public’s awareness of, and comfort with, these services — all hastened by the COVID-19 Federal Public Health Emergency.
The U.S. Congress and the Centers for Medicare and Medicaid Services (CMS) used its authority during the PHE to significantly expand Medicare coverage for virtual care services, covering telehealth visits in urban areas and from patient’s homes. In addition, Medicare began covering a wide range of clinical services virtually such as behavioral health and physical therapy; it also expanded coverage for different service delivery modalities to include audio-only visits. As a result of the changes, Medicare became a leading payer for virtual care nationally between 2020 and 2022. Over this same period, private insurers and state Medicaid programs largely followed Medicare’s lead by expanding their own virtual care coverage.
One of the consequences of the PHE is that most payers have embraced Medicare’s basic definitional structure for types of virtual care services. As a part of this typology, virtual care services are divided into two general buckets of services: telehealth visits (physician office visits conducted via audio and video technology), which are typically prohibited by statute in urban areas or a patient’s home; and Communication Technology-Based Services (CTBS) which can be conducted anywhere. CTBSs include: remote patient monitoring (RPM); virtual check-ins (brief patient-to-clinician exchanges); e-visits (online portal or email visits); and e-consults (clinician to clinician interaction).
With the end of the PHE on May 11, Medicare coverage of virtual care services and coverage offered by other payers will change. The details and scope of this change have many stakeholders concerned and confused. HMA has a keen sense for which virtual care services may get a new lease on life in the coming months and which are likely to be hotly debated in the years ahead. The one certainty is that the last 3 years have altered the landscape for virtual care services for years to come.
Shift in Virtual Care Landscape
As a result of the statutory geographic limitations and restrictions placed on traditional fee-for-service (FFS) Medicare coverage, use of telehealth services was minimal most of the last decade, with only one-quarter of 1 percent (0.25%) of beneficiaries in FFS Medicare using virtual care services.[1] Even among Medicare Advantage plans and Medicare Accountable Care Organizations (ACOs), neither of which which face the same restrictions, virtual care was utilized very rarely before 2019.
This sluggish use of telehealth was radically altered when HHS used its PHE authority to relax constraints on the use of use virtual care services by Medicare beneficiaries and providers.[2],[3] Among the most consequential changes made by policymakers at the outset of the PHE were:
Enabling telehealth services to be provided anywhere (e.g., urban areas and patients’ homes);
Allowing Federally Qualified Health Centers (FQHC) and Rural Health Clinics (RHC) to conduct virtual care services;
Granting various types of clinicians permission to deliver virtual care services;
Enabling new patients to receive virtual care services;
Authorizing audio-only services;
Permitting telehealth services for more than 200 different types of clinical services (e.g., mental health, emergency department, physical and occupational therapy, critical care, inpatient care);
Relaxing HIPPA rules to enable the broad use of smartphones for virtual care.
Due to these policy changes, rates of virtual care skyrocketed during the PHE (Figure 1). In April of 2020 the number of Medicare claims for any type of virtual care service exceeded 9 million, while 2019 the number of these services provided monthly never exceeded 100,000 (Figure 1). On an annual basis, from 2019 to 2021 the number of virtual care visits jumped from roughly 1 million to 39 million and the number of unique beneficiaries receiving these services increased from 300,000 to nearly 12 million.
Figure 1: Number of Virtual Care Service Visits, Number of Unique Medicare Fee-For-Service Beneficiaries, and Number of visits per Utilizer by Month, December 2019 to December 2021.
Source: HMA analysis of CMS’s 100 percent Medicare Fee-For-Service Claims data for 2019, 2020, and 2021.
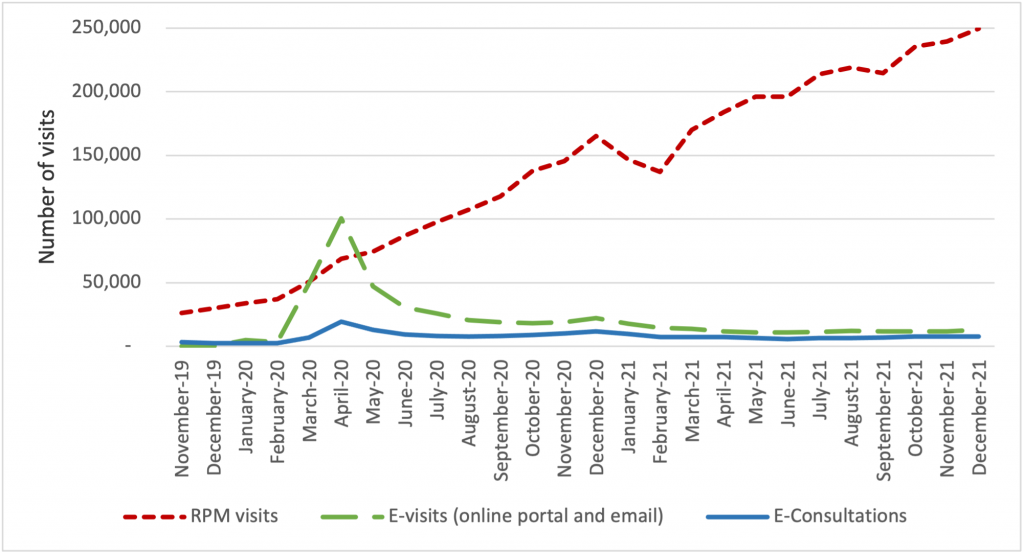
The growth of virtual care services has largely been driven by an increase in telehealth visits, but we observe important trends in the use of CTBSs, as well. In late 2021, more than 90 percent of visits were associated with telehealth, while 10 percent were associated with CTBSs. Early in the PHE, all of these service types experienced an initial, abrupt increase in use (Figure 2). By contrast, the growth in the use of remote patient monitoring (RPM) has been continuous since 2020. The growth in use of RPM reflects the general movement of services into patients’ homes and has been accelerated by specialist such as cardiologists and endocrinologists beginning to leverage the power of RPM. We expect greater diffusion and use of RPM and other CTBSs in the next five years.
Figure 2: Number of Virtual Care Service Visits for Remote Patient Monitoring, Virtual Check-ins, E-visits, and E-Consultations by Month, December 2019 to December 2021.
Source: HMA analysis of CMS’s 100 percent Medicare Fee-For-Service Claims data for 2019, 2020, and 2021.
Policies temporarily in place until the end of 2024
During the PHE, Congress made critical long-term changes to Medicare’s coverage of virtual care services that continued to spur the use of these services and offer access to care for beneficiaries. In 2021, Congress changed the law to permanently allow Medicare beneficiaries to receive behavioral/mental telehealth services regardless of location (urban or rural) and for this care to be available to patients in their own homes.
In 2022, Congress severed the link between the PHE declaration and Medicare coverage policies for virtual care services, extending those benefits through the end of calendar year 2024. We expect that coverage for all telehealth services will receive considerable attention from federal policymakers and stakeholders towards the end of 2024.
Immediate impact of expiring policies
Certain aspects of Medicare’s virtual care policies will, however, terminate May 11, 2023, when the PHE declaration comes to an end. Several of the expiring policies have a broader impact beyond the Medicare program, affecting patients insured by private payers and State Medicaid programs.
Specifically, when the PHE ends, policymakers will need to address the following anticipated changes:
The Office for Civil Rights (OCR) will return to imposing penalties on providers who violate the provisions of the Health Insurance Portability and Accountability Act (HIPAA) by using public-facing remote communication technologies which are not HIPAA-compliant. This may prohibit the use of some of the most common smartphone-based video conferencing tools for health care visits.
Medicare beneficiaries without an existing relationship with a clinician will be unable to receive CTBSs such as RPM, virtual check-ins, and e-visits.
Providers will no longer be allowed to provide virtual care services across state lines, because most state medical licensure boards will return to pre-PHE policy.
Federal rules from the Drug Enforcement Agency (DEA) may revert to the pre-PHE requirement that clinicians establish a patient-provider relationship in-person before being permitted to prescribe controlled substances for substance use disorder treatment.
Potential policy changes occurring before 2025 As explained earlier, Medicare coverage for many virtual care services will remain in place for the next 19 months. Before the end of 2024, Congress will need to address several policy questions, and among the most widely debated are whether to:
Restore Medicare’s statutory prohibition on telehealth services being delivered in urban areas or in home settings;
Allow Federally Qualified Health Centers and Rural Health Clinics to provide telehealth services to Medicare beneficiaries; or
Continue to cover audio-only telehealth visits under Medicare.
Lawmakers will look to payers, patients, and providers for feedback before making these policy decisions. Among the most critical pieces of information they will also consider will be the results of the study Congress has required of HHS regarding trends in the use of virtual care. This study’s final report is due in 2026, which has led some to speculate that Congress will delay action on virtual care coverage policy until then. In the meanwhile, we expect HHS will be assessing the overall volume of virtual care use, who is using which types of services, and the levels of related fraud and abuse.
Looking Ahead
In the United States, our experience during the acute phase of the pandemic demonstrated that patients and providers are more receptive than previously thought to utilizing digital technologies for the delivery of care. This experience may also influence policymakers’ decisions about reimbursement and coverage of wearable devices, as well as other cutting-edge tools that rely on artificial intelligence or machine learning.
HMA believes payers and providers alike can take steps now to strategically prepare for the still evolving and growing landscape of digital health care.
Based on the various changes that have occurred in the virtual care environment over the last 3 years, we are intently watching several areas of potential change in the practice of medicine and the ways payers set coverage policy. Below are some of the trends we anticipate in the years ahead:
Continued use of virtual care services at levels observed in 2021.
An expansion of CMS’s programs to protect against fraud and abuse related to virtual care.
Notable growth in the use of RPM, and related services for physical and occupational therapy services.
The proliferation of innovative home-based screening and testing technologies. We anticipate payers will encourage the use of these at-home tests for things like kidney function, liver function, and colorectal cancer screening in order to limit care delivery in higher cost settings.
Growth in “virtual-first” insurance plans, where patients are encouraged to use virtual care first – prior to being seen in person. As these plan options expand, we anticipate virtual care use will rise, and reimbursement rates will begin to change.
Virtual care services are primed for additional growth and HMA is working with a wide variety of payers, providers, and foundations to develop strategies for adapting to state and federal rules and regulations related to virtual care. Changes in this landscape will hinge on research CMS will complete by the end of 2026, and coverage decisions made by states and commercial payers. HMA is well positioned to assist stakeholders with work in this area and can leverage access to Medicare and Medicaid claims data to conduct health services research to illustrate geographic variations in the use of virtual care.
If you have questions on how HMA can support your agency before or after the end of the PHE, please contact our experts below.
[2] Centers for Medicare & Medicaid Services. Medicare telemedicine health care provider fact sheet. March 17, 2020. https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet
[3] HHS Administration for Strategic Preparedness & Response (ASPR). https://aspr.hhs.gov/legal/PHE/Pages/default.aspx
HMA’s 3-part New Rules in Treatment of Opioid Addiction webinar series is aimed at helping stakeholders prepare for new federal rules that will change how medications are delivered to persons with opioid use disorders. Reducing daily visits will allow persons served to engage in work, family and community activities that sustain recovery, but programs have historically relied on daily visits for revenue. With the new rules, opioid treatment centers (OTPs) have a unique opportunity to advance person-centered care. In part 1 of this series, we addressed changes in clinical and business practices, as well as payment structures that will enable OTPs to implement new treatment programs and other flexibilities to improve patient outcomes. Other parts of the webinar series examine policy and incentives in the new system.
Learning Objectives
OTP Regulatory Changes – Understand expected changes from the point of view of clinicians and providers.
Critical Action Steps – Identify what OTPs will need to do next to comply.
State Variation – Consider how to navigate new rules across states with different approaches to treatment.
This week, our In Focus section reviews CMS’s proposed changes to the federal Medicaid managed care access, finance, and quality regulation (CMS-2439-P). A future In Focus will take a closer look at the proposed changes to the federal Medicaid access to care regulation (CMS-2442-P), which also has significant implications for state Medicaid programs.
On April 28, 2023, the Centers for Medicare & Medicaid Services (CMS) unveiled two significant and related proposed rules addressing Medicaid managed care access, finance, and quality requirements. Together these proposed rules signal a new era of accountability and transparency in the Medicaid program. They also strengthen beneficiaries’ role in influencing the policies and administration of state Medicaid programs.
Table 1 identifies a few of the key themes and issues addressed in the Medicaid managed care proposed rule. The deadline for submitting comments to CMS is July 3, 2023.
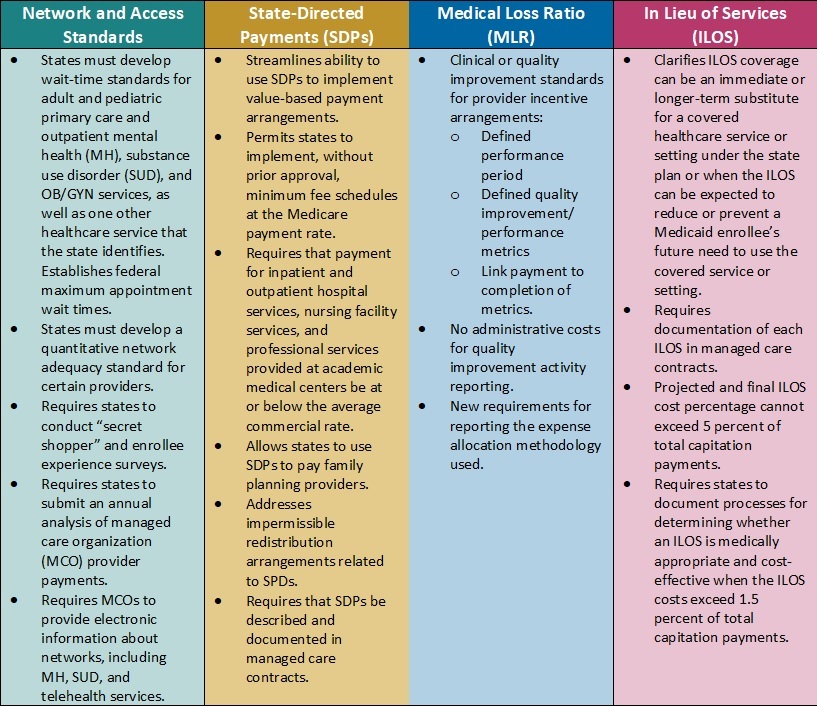
Table 1. Medicaid Managed Care Proposed Rule: Snapshot of Proposed Changes
Key Themes and Considerations
Payment Ceilings May Accelerate Value-Based Payment Arrangements. Current federal regulations allow states to direct managed care organizations (MCOs) to pay providers according to specific rates or methods. States have used these directed payment arrangements to set minimum payment rates for certain types of providers or to require participation in value-based payment (VBP) initiatives.
In the proposed rule, CMS calls for establishing an upper limit for these payments. Specifically, the agency plans to limit the projected total payment rates to the average commercial rate (ACR) for inpatient and outpatient hospital services, nursing facility services, and qualified practitioner services at academic medical centers that states include in state-directed payment (SDP) arrangements. The ACR limit, in concert with the proposed SDP documentation and reporting, is among the most significant and complex proposed changes in the rule.
Considerations: The proposed changes represent a strong federal regulatory push to accelerate movement to VBP in Medicaid, which provides states with new levers to drive value in their Medicaid delivery systems. It also means that MCOs, providers, and other stakeholders will need to navigate and help inform the policies and contractual arrangements that will flow from the pending changes. For example, states may need to reflect on the following considerations:
Whether the proposals will require them to reduce reimbursement
Whether they will need to develop new value-based arrangements through SDPs and how these policies will be structured
What outcomes they might need to prioritize
How transparency in reporting provider-level payments could affect non-federal funding and SDP initiatives
Updated Approach to in Lieu of Services (ILOS) Facilitates Whole-Person Care. In January 2023, CMS issued a State Medicaid Director Letter (SMDL#23-001) advising states of the option to use the ILOS authority in Medicaid managed care programs to reduce healthcare inequities and address unmet health-related social needs (HRSNs), such as housing, food insecurity, and intimate partner violence. The proposed Medicaid managed care rule would expand upon and codify in regulation that guidance.
Considerations: Although the ILOS proposal adds reporting requirements and guardrails to address fiscal accountability, overall, the updated policy signals CMS’s willingness to support innovative state approaches to meet a continuum of beneficiary needs, including HRSNs that affect the social drivers of health. Notably, CMS advises that the substitution of an ILOS for a state plan service or setting should be cost-effective but does not need to be budget-neutral. States also can specify that an ILOS can be an immediate or longer-term substitute for a state plan service or setting.
States could pursue a variety of options under CMS’s revised ILOS framework. State Medicaid agencies and their partners can collaborate on ILOS strategies that will allow them to make further progress toward reducing healthcare inequities, as well as fulfill their quality strategy goals and objectives.
New Standards for Medical Loss Ratio Strengthen Link to Performance Improvement. Existing federal regulations require Medicaid managed care plans to report their medical loss ratio (MLR) to states annually, and, in turn, states must submit a summary of those reports to CMS. Many state MCO contracts require plans to comply with provider incentive and bonus policies; however, MCOs infrequently make incentive payments contingent on the provider meeting quantitative clinical or quality improvement standards.
Consistent with the healthcare sector’s transition toward value-based care, CMS proposes to strengthen the link between an MCOs incentive payment to a provider and the provider meeting defined quality improvement or performance metrics. Additionally, contractual language between MCOs and providers will need to more explicitly identify the dollar amounts tied to successful completion of these metrics. Only incentive payments based on quality improvement will be considered incurred claims when plans calculate their MLR; administrative costs cannot be included in quality improvement activity reporting.
Considerations. The proposed requirements are expected to add more transparency to negotiations between Medicaid MCOs and providers. MCOs will retain flexibility to determine the quality improvement or quantitative performance metrics, which carry more weight and accountability in CMS’s revised regulatory framework.
Network Adequacy Requirements Strengthen Link to Access and Rates. CMS also proposes policies that the agency believes will help strengthen Medicaid enrollees’ access to services. For example, the rule would require states to develop wait-time standards for adult and pediatric primary care and outpatient mental health, substance use disorder (SUD), and OB/GYN services, with CMS establishing federal minimum appointment wait times. States also will need to develop a quantitative network adequacy standard, beyond wait times, for certain providers.
Notably, CMS also plans to require states to submit an MCO-level analysis of MCO-to-provider payments. This analysis may provide more insights about the relationship between rates and access to certain types of providers and services. It may also improve alignment in access policies across delivery systems.
Considerations: States and MCOs should expect to need more sophisticated analysis of provider capacity at state and local market levels. This information will be critical in developing network adequacy standards and determining where additional provider support may be necessary. Expanded and new strategies may be needed to ensure compliance with the federal rules and resulting changes to state policies.
What’s Next
Many of CMS’s proposals track closely with many recent recommendations from federal commissions and oversight entities, including the Medicaid and CHIP Payment and Access Commission (MACPAC) and Government Accountability Office (GAO), which may indicate a greater likelihood that CMS will finalize those policies. If they are finalized largely as proposed, the rule will further the Biden Administration’s directional imprint on the Medicaid program.
Within the proposed rules described above, CMS identifies numerous areas where stakeholder input would be beneficial. States, MCOs, providers, and other interested stakeholders should analyze the proposals and consider submitting comments to CMS on the feasibility, potential impact, and, where applicable, alternatives to the proposed changes. Stakeholders also may use this time to begin planning for 2024 and determining what resources and tools they may need to prepare for implementation of the final regulations, as well as how their approach may vary based on state-specific factors.
For questions about the rule and how HMA’s team of experts can support your organization’s response, please contact our experts below.
HMA’s five-part 1115 Justice Waivers: Building Bridges of Health for Persons Leaving Carceral Settings webinar series is designed to help plans and other stakeholders improve the long-term health outcomes of individuals leaving carceral settings. This webinar focused on the carceral settings operational healthcare practices, including intake screenings to aid in risk assignment and facilitate community re-entry. The 1115 justice waivers allow Medicaid programs to support in-carceral care, but to optimize resources, systems need information to translate transition in care best practices to carceral places of service.
HMA consultants with lived leadership experience working inside and outside jails and prisons provided plans and state agencies with a unique perspective on opportunities for transformation.
Learning Objectives:
Establishing Health Care Transitions Across Providers: Methods to improve transitions in care through recognizing carceral facilities as a place of service in the continuum of care.
Health Risk Assessments to Improve Continuity of Care: Utilizing health screening and risk assessments done at intake and throughout incarceration so Medicaid can improve healthcare transitions from jail into the community.
Other webinars in the “1115 Justice Waivers: Building Bridges of Health for Persons Leaving Carceral Settings” series:
This week our In Focus section reviews guidance from the Centers for Medicare & Medicaid Services (CMS), released on April 17, 2023, encouraging states to apply for the new Medicaid Reentry Section 1115 Demonstration Opportunity. The demonstration is aimed at helping improve care for individuals in carceral settings prior to their release.
Background
The United States has approximately 1.9 million individuals incarcerated nationwide. Studies have shown higher rates of mental illness and physical health care needs in incarcerated populations compared to the general population, as well as associations between jail incarceration and increases in premature death rates from infectious diseases, chronic lower respiratory disease, drug use, and suicide.
CMS states that formerly incarcerated individuals with physical and mental health conditions and substance-use disorders (SUDs) typically have difficulty succeeding upon reentry due to obstacles present immediately at release, such as high rates of poverty and high risk of poor health outcomes. These individuals tend to face barriers in obtaining housing, education, employment, and health care access upon release. They often do not seek outpatient medical care and are at significantly increased risk for emergency department (ED) use and hospitalization.
Purpose and Goals
After collecting feedback from stakeholders, including managed care organizations, Medicaid beneficiaries, health care providers, the National Association of Medicaid Directors, and other representatives from local, state, and federal jail and prison systems, CMS designed the Reentry Section 1115 Demonstration Opportunity. The services covered under this demonstration opportunity should aim to improve access to community resources that address the health care and health-related social needs of the carceral population, with the aims of improving health outcomes, reducing emergency department visits, and inpatient hospital admissions for both physical and behavioral health issues once they are released and return to the community.
The purpose of this demonstration opportunity is to provide short-term Medicaid enrollment assistance and pre-release coverage for certain services to facilitate successful care transitions. The full goals, as quoted from CMS, are as follows:
“Increase coverage, continuity of coverage, and appropriate service uptake through assessment of eligibility and availability of coverage for benefits in carceral settings just prior to release
Improve access to services prior to release and improve transitions and continuity of care into the community upon release and during reentry
Improve coordination and communication between correctional systems, Medicaid systems, managed care plans, and community-based providers
Increase additional investments in health care and related services, aimed at improving the quality of care for beneficiaries in carceral settings and in the community to maximize successful reentry post-release
Improve connections between carceral settings and community services upon release to address physical health, behavioral health, and health-related social needs
Reduce all-cause deaths in the near-term post-release
Reduce number of ED visits and inpatient hospitalizations among recently incarcerated Medicaid beneficiaries through increased receipt of preventive and routine physical and behavioral health care”
CMS encourages states to engage with individuals who were formerly incarcerated when contemplating the design and implementation of their proposal. CMS also encourages states to design a broadly defined demonstration population that includes otherwise eligible, soon-to-be former incarcerated individuals. States have the flexibility to target population, such as individuals with specific conditions, but are encouraged to be mindful of undiagnosed conditions. States should have a plan to ensure incarcerated individuals will be enrolled in Medicaid upon their release, applying for Medicaid no later than 45 days before the day of release.
Reentry Section 1115 Demonstration Opportunity
To receive approval for the demonstration, the state proposal must include in the pre-release benefit backage:
Case management to assess and address physical and behavioral health needs and health-related social needs;
Medication-assisted treatment (MAT) services for all types of SUD as clinically appropriate, with accompanying counseling; and
A 30-day supply of all prescription medications that have been prescribed for the beneficiary at the time of release, provided to the beneficiary immediately upon release from the correctional facility.
In addition to these three services states may include other important physical and behavioral health services to cover on a pre-release basis, such as family planning services and supplies, behavioral health or preventive services, including those provided by peer supporters/community health workers, or treatment for Hepatitis C. CMS is also open to states requesting Section 1115 expenditure authority to provide medical supplies, equipment, and appliances.
The Reentry Section 1115 Demonstration opportunity is not intended to shift current carceral health care costs to the Medicaid program. CMS will not approve state proposals to receive federal Medicaid matching funds for any existing carceral health care services funded with state or local dollars unless the state agrees to reinvest the total amount of new federal matching funds received into activities or initiatives that increase access to or improve the quality of health care services for individuals who are incarcerated.
CMS also expects states to refrain from including federal prisons as a setting in which demonstration-covered prerelease services are provided under the opportunity.
States with approved demonstrations will need to submit an implementation plan, a monitoring protocol, quarterly/annual monitoring reports, a mid-point assessment report, an evaluation design, and interim/summative evaluation reports.
California
California became the first state to receive approval for a Section 1115 waiver amendment earlier this year to provide limited Medicaid services to incarcerated individuals for up to 90 days immediately prior to release. The approval period runs through December 31, 2026, timed with the expiration of the CalAIM Medi-Cal waiver demonstration. California’s reentry demonstration initiative aims to provide health care interventions at earlier opportunities for incarcerated individuals to reduce acute services utilization and adverse health outcomes. The state anticipates it will increase coverage and continuity of coverage for eligible beneficiaries, improve care transitions for beneficiaries as they reenter the community, and reduce morbidity and mortality in the near-term post-release.
Pre-release services include comprehensive care management, physical and behavioral clinical consultation, lab and radiology, MAT, community health worker services, and medications and durable medical equipment. A care manager will be assigned to eligible individuals to establish a relationship, understand their health needs, coordinate vital services, and make a plan for community transition, including connecting the individual to a community-based care manager they can work with upon their release. Additionally, all counties implementing Medi-Cal application processes in jails and youth correctional facilities will “suspend” the Medicaid status while an individual is in jail or prison, so that it can be easily “turned on” when they enter the community.
On April 6, 2023, HMA held a webinar titled, “Medicaid authority and opportunity to build new programs for justice-involved individuals.” The webinar replay is now available. HMA will announce additional webinars on the topic.