Leticia Reyes-Nash is a principal in HMA’s community strategies practice and an expert in healthcare equity and innovation in healthcare service delivery. Leticia shares her inspiring journey from political and community organizing to her work in health policy, highlighting the importance of addressing health equity and the challenges within healthcare systems. She discusses strategies for integrating equity into business practices, emphasizing the need for continuous quality improvement, humility, and patience in healthcare initiatives.
391 Results found.

What would it take to make the ACA more affordable?
Liz Wroe is a principal at Leavitt Partners DC office and former Senate health policy director. Liz talks about the evolution of the Affordable Care Act (ACA), sharing her experiences during the ACA’s passage, repeal efforts, and stabilization of the individual market. She discusses challenges in bending the cost curve, the impact of ACA subsidies and silver loading, and the need for more honest conversations in healthcare policy.

HMA 2024 Spring Workshop summary and key takeaways
On March 6, HMA convened a spring workshop of 100 healthcare stakeholders interested in making value-based care delivery and payment work better. This event was designed for those engaging in value-based care and payment transformation, but who are looking to learn from peers to overcome challenges; participants included insurers, health systems, data and tech innovators, service providers, and trade associations.
The event’s name implored people to “Get Real” about the challenges we all face, while reminding ourselves of the imperative of making this transition to ensure the sustainability of our uniquely American healthcare system. In between plenary panels, participants were engaged in cohort discussions exploring the opportunities for progress in areas critical to making value-based care work. While a summary cannot recreate the real-time discussions and simulations from the event, our discussions delivered insights on several critical themes that we believe are important to track.
EMPLOYERS ARE LEANING IN: For all employers pay, they are getting less value over the past decade; the changes made to ERISA that hold the C-suite accountable for paying fair prices for healthcare benefits is a seismic shift in making healthcare purchasing a more strategic priority for employers.
- Elizabeth Mitchell of the Purchaser Business Group on Health illustrated the shift in employers’ awareness – due to data transparency rules – that they aren’t getting the quality they thought they were getting for all that they pay. Transparency, plus a recent change to the Employee Retirement Income Security Act of 1974 (ERISA), is bringing employers back to the table with very specific requests for better outcomes, which they are increasingly pursuing through direct contracting and specific quality frameworks for primary care, maternal care, and behavioral health. Participants continued to reflect on this dynamic in all subsequent discussions, underscoring that this could be a really big deal.
- Cheryl Larson of the Midwestern Business Group on Health talked about the cost pressure on her members leading them to partner in new and different ways, expressing optimism about all payer solutions and other innovative approaches to leverage the cost data that are now available. In her closing plenary session, she said “this issue of accountability on employers…I am excited and optimistic that there are things we can do to get there faster now.”
Data & Technology HAVE TO IMPACT DECISION MAKING: Patients are using the system the way it is designed today, so we can’t just blame them for poor outcomes…we have to actually stop doing things that don’t work and start measuring things the right way.
- Dr. Katie Kaney opened with a dinner keynote discussing her efforts to create metrics that give purchasers a better measurement of whole person care, including clinical, genetic, behavioral, and social factors. Audience members remarked that this was a novel approach to quantify what has become accepted correlation in adverse health outcomes.
- Ryan Howells, Dave Lee, and Stuart Venzke led discussions on Data & Technology, diving into updated federal regulations that present both opportunities and challenges for stakeholders, as well as ways to create corporate strategies that include data and technology, as these issues are no longer optional for anyone in this business. The breakout discussions talked about where we are today vs where we need to be – bridging the gap between data and decision making.
Payment & Risk TOOLS ARE ALIGNING INFORMATION TO ACTION: Achieving meaningful risk-based contracts is possible but the details matter…mismatched data and information leads to unequal buying power, which cannot be the case in value-based care.
- Kelsey Stevens, Scott Malan, Hunter Schouweiler, and Kate de Lisle led discussions on Payment & Risk, including an exciting hands-on simulation exercise that helped participants understand ways to increase premium scores by implementing risk-based payment approaches within the care delivery system; this session provided very concrete takeaways for those who attended by combining a simulation with a discussion on measures of success to improve risk-based contracting strategies.
- Amy Bassano and Kate de Lisle discussed their recent publication on the expanded ecosystem of value-based care entities, looking at the “enablers” who are working with providers and payers to manage risk. This groundbreaking landscape of this market segment highlighted a set of Guiding Principles to ensure these entities are aligned with CMS, provider, and patient goals. Participants had lots of questions for the presenters and were anxious to read the HMA full report.
CARE DELIVERY MEASURES MUST BE TANGIBLE TO PROVIDERS AND PATIENTS: Value-based care requires aligning the right metrics with the right incentives, ensuring providers understand not only WHY but HOW they help improve patient outcomes.
- Rachel Bembas, Dr. Jean Glossa, and Dr. Elizabeth Wolff led discussions on Care Delivery Measures, underscoring the importance of involving clinicians in the establishment of outcomes measures, as well as ensuring that the diversity of patient experiences are included. Participants remarked that we have a lot of “messy” data today, so we now have to ask the next set of questions on how we best use the messy data to make an impact?
- Former Congresswoman Allyson Schwartz talked about the continuing promise of Medicare Advantage, and the opportunity to convene a new alliance around Medicare quality metrics as well as the increasing pressure to align these metrics across payers. In the closing plenary, she said “We need to define what we want healthcare in America to look like and then go out and get it…. We have to align the measurements and the standards we use so that providers understand what’s needed and it benefits government, taxpayers, and beneficiaries…we should require plans to have risk-based contracting with providers.”
Policy & Strategy HAVE TO STAY THE COURSE TO ALIGN INCENTIVES: Policymakers can help or hinder movement forward to ensure success…value-based care has to be more than a section in an RFP, but part of the entire scope of paying for outcomes-based care delivery.
- Governor and former HHS Secretary Mike Leavitt reminded us of the political and policy journey that got value to where it is today, and the unique moment we are in right now that gives us hope as we enter this post-pandemic phase of healthcare spending and policy. He reflected, “We are beginning to see regulations and mechanisms to hold people accountable for healthcare costs…we have to integrate value and caregiving or we will never get to value.”
- Theresa Eagelson, former Illinois Director of Healthcare and Family Services, talked about the opportunity for states to expand value-based care by setting strong expectations through contracting and by thinking differently about policy choices. She reflected on the role of state administrators, “When we sit here and talk about value-based care, do we know what our north star is? Have we mastered what we want to see in RFPs (for Medicaid)? We’re working on a good FQHC model in Illinois, but should it be just for FQHCs? We need to spend more time together, across payers, across plans and providers and consumers to figure out what success looks like.”
- Caprice Knapp and Teresa Garate led a discussion on state and local Policy & Strategy to support integrated care and services that are required to achieve better outcomes. There is a need for services to better coordinate and manage care across social and health services, bringing contracting and payment expertise to more efficiently serve patients. The highly anticipated Medicaid managed care rule can help guide states in updating their approach. Federal analysis of Medicaid data is needed to set benchmarks before we can get to total cost of care approaches.
- Amy Bassano and AnneMarie Lauterbach led a discussion on federal policy alignment of Medicare FFS and Medicare Advantage, particularly looking at drug spending and the very real burden of medical debt as a driver of policy change. Participants reflected that half the country is indirectly covered through some public insurance. It’s just being done hyper-inefficiently.
HMA is leading the way on value-based care and is committed to continuing these dialogues to drive local, state, and national change. HMA’s value-based care expertise draws from our acquisition of Leavitt Partners and Wakely Consulting Group, two firms with deep ties and expertise on policy, strategy and risk-based pricing strategies, as well as recruitment of clinicians and operational experts who have led organizations through this transition. We will continue to advance the dialogue – and the work – to drive value as a critical way to ensure that our systems of health and healthcare are more affordable, equitable, and sustainable.
Let’s keep the conversation going! Click here to learn more about how HMA can help you succeed with value-based payments and check out the newly released value-based payment readiness assessment tool for behavioral health providers.
State teams convene to strengthen collaboration across child welfare, behavioral health, and Medicaid
This week, our In Focus section highlights the Children’s Behavioral Health (CBH) State Policy Lab, held February 7−9, in Baltimore, MD. Health Management Associates, Inc., (HMA), in partnership with national philanthropies and associations, hosted the Policy Lab, which provided an unprecedented opportunity for state cross-systems teams to conduct in-depth work toward creating an equitable behavioral health system of care for children and youth.
Background
The lack of collaboration and misaligned strategies and policies across state child welfare, behavioral health, and Medicaid has contributed to unsatisfactory outcomes for children and youth in our communities. The COVID-19 public health emergency exacerbated these issues, as the rate of mental health and substance use disorders (SUD) increased and many families experienced traumatic events during this time. Increasingly, states and local jurisdictions are exposed to threats or actual class action lawsuits based on the inadequate care of children and youth involved in the child welfare settings.
Fortunately, federal and state efforts and investments to address the youth systems of care—including schools, community, delivery systems, and community-based child placing agencies—are in motion. Though the diversity of efforts being implemented across local and state agencies are critical, these complex issues require collaboration across multiple systems, including Child Welfare, Behavioral Health authorities, Medicaid, and K-12 Education. A cross-sector strategic approach will enable comprehensive identification of gaps, policy solutions, and best practices, as well as highlight opportunities for cross-sector braided or blended funding to build a system of care that supports the needs of multi-system children, youth, and their families.
Child Behavioral Policy Lab
The current behavioral health crisis presents an opportunity to address long-term challenges and divisions and to build a truly comprehensive approach. This is why HMA sponsored the Children’s Behavioral Health State Policy Lab which convened key partners within a state and across states. The Annie E. Casey Foundation, Casey Family Programs, National Association of State Mental Health Program Directors (NASMHPD), the Child Welfare League of America (CWLA), the American Public Human Services Association (APHSA), National Association of Medicaid Directors (NAMD) and MITRE, a Children’s Behavioral Health (CBH) State Policy Lab, joined HMA in funding, organizing and providing consultation support for the meeting.
The nine participating states—Georgia, Kansas, Kentucky, Maryland, Missouri, Pennsylvania, Texas, Utah, and Wisconsin—were selected through a competitive process based on the goals and commitment of the state and the thorough analysis of gaps and opportunities, demonstration of collaborative state interagency partnerships, and engagement of youth and adults.
The participating states committed their leadership teams to join the Policy Lab in laying the foundational work of development of statewide plans that would advance their collective goal of creating a more united system of care. Participants learned about intergenerational trauma and resilience. The sessions also provided participants with data that helped provide context to the problems we are trying to solve. Presenters included Aliyah Zeien, a national child welfare policy advocate and youth ambassador, with lived experience who highlighted that 25 percent of foster youth will spend time in prison or other enforcement systems within two years of leaving the child welfare system. Her experience and reflections served as call for action to actively engage families and youth in all system planning, advocacy, and policy work.
Key areas of focus
Following these brief educational sessions, each state had substantial “team time” to develop a road map and set of next steps for continuing their work after the Policy Lab. Expert facilitators guided state teams through discussions on three key issues:
- Service array. State teams were challenged to define their array of services and develop collective agreements on how to develop enhanced treatment options for children and their families. With an emphasis on building a full continuum of care with community-based supports and fewer children in residential facilities, each team considered challenges such as eligibility, access, and workforce. Prevention, diversion, and engagement of people with lived experience to help with system development were common commitments in state action teams.
- Financing. The teams considered their statutory authority, funding streams, funding partners, contract vehicles, and financing mechanisms. They also worked on ideas for blending and braiding funding, with a focus on Medicaid and leveraging collective opportunities to develop staff and contractual resources.
- Governance. State teams worked through difficult conversations, including how to measure success, how to manage accountability and monitoring, how to collaboratively design services and case practice, while meaningfully sharing data and creating interoperability within their systems while respecting confidentiality and privacy concerns.
What’s Next
Since the Policy Lab program, most participating states have embarked on next steps identified during the workshop, such as vetting their plans with state leadership, creating an ongoing team for implementation, and identifying community partners. HMA and HMA Companies, including Leavitt Partners, are collaborating with our Policy Lab partners and the state agencies to further develop these plans and prepare for implementations that rethink our approach to services for youth and their families.
For more information about the Policy Lab and follow-on work, please contact Uma Ahluwalia ([email protected]), Christina Altmayer ([email protected]), Jon Rubin ([email protected]), and Sarah Scholle ([email protected]).
Federal policymakers consider current and future spending measures on simultaneous tracks
This week, our In Focus section covers Congress’s and the Administration’s parallel efforts to finalize fiscal year (FY) 2024 spending bills and begin the budget process for FY 2025.
Congress approved a bipartisan package for some of the FY 2024 spending bills, and on March 9, 2024, President Biden signed the Consolidated Appropriations Act of 2024 into law (PL 118-42). Programs funded through this measure include the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and other federal nutrition supports, rental assistance for safe and affordable housing, and veterans medical care and benefits.
Several mandatory funding extensions of public health programs and health-related policies also found their way into the 2024 consolidated appropriations package, including extending the Community Health Center Fund, delaying reductions in the disproportionate share hospital allotments, defining Certified Community Behavioral Health Centers (CCBHCs) as a Medicaid service, extending incentive payments for certain Medicare providers, and mitigating the impact of cuts to the Medicare physician fee schedule.
These policies, however, addressed a narrower set of issues than the expansive and bipartisan legislation that has been moving through both chambers of Congress. For example, House and Senate members have worked on respective bipartisan policies affecting price transparency, pharmacy benefit managers, and Medicare site-neutral policies, among others.
Meanwhile, President Biden released the FY 2025 Budget proposal March 11, 2024, kicking off the annual budget process. Like the administration’s FY 2024 budget proposal, the FY 2025 plan emphasizes deficit reduction and continues to make equity and Medicare solvency cornerstones of the budget. Health-related priorities include expanding access to affordable healthcare services, lowering drug costs, improving maternal health, addressing the mental health and substance use disorder crises, and enhancing biodefense and preparedness activities.
Check out the FY 2025 budget analysis from Leavitt Partners, a Health Management Associates, Inc. (HMA), company, here, and a deeper dive into the Consolidated Appropriations Act of 2024 here.
What We’re Watching
Congress is continuing negotiations on the outstanding spending bills, including the one that funds the Departments of Health and Human Services, Labor, and Education through September 2024. Lawmakers are working to reach an agreement before the next funding deadline of March 22.
The administration’s FY 2025 budget proposals are generally being characterized as a blueprint for President Biden’s re-election campaign and, if successful, a policy agenda for his second term. Though Congress has already begun holding hearings on the budget request, members on both sides of the aisle will likely focus on issues that resonate in an election year.
Regardless of the outcome of the November elections, Congress has an opportunity to address unfinished business during the lame duck session later this year.
HMA and Leavitt Partners collaborate to monitor legislative and regulatory developments in healthcare and adjacent spaces and to assess the impact of policy changes on the healthcare industry.
Medicaid managed care spending in 2023
This week, our In Focus section analyzes preliminary 2023 Medicaid spending data collected in the annual CMS-64 Medicaid expenditure report. After submitting a Freedom of Information Act request to the Centers for Medicare & Medicaid Services (CMS), HMA received a draft version of the CMS-64 report that is based on preliminary estimates of Medicaid spending by state for federal fiscal year (FFY) 2023. Based on the preliminary estimates, Medicaid expenditures on medical services across all 50 states and six territories in FFY 2023 totaled nearly $852.9 billion, with 59.6 percent of that amount now flowing through Medicaid managed care programs. In addition, total Medicaid spending on administrative services was $33.8 billion, bringing total program expenditures to $886.7 billion.
Total Medicaid Managed Care Spending
Total Medicaid managed care spending (including the federal and state share) in FFY 2023 across all 50 states and six territories was $508.1 billion, up from $468.3 billion in FFY 2022. This figure includes spending on comprehensive risk-based managed care programs as well as prepaid inpatient health plans (PIHPs) and prepaid ambulatory health plans (PAHPs). PIHPs and PAHPs refer to prepaid health plans that provide only certain services, such as dental or behavioral health care. Fee-based programs such as primary care case management (PCCM) models are not included in this total. Following are some key observations.
- Total Medicaid managed care spending grew 8.5 percent in FFY 2023.
- Managed care spending growth has decreased in since the end of the COVID-19 pandemic, after peaking in FFY 2021.
- In terms of dollars, the increase in Medicaid managed care spending from FFY 2022 to FFY 2023 was $39.8 billion, compared with $47.8 billion from FFY 2021 to FFY 2022.
- Medicaid managed care spending has increased at a compounded annual growth rate (CAGR) of 14.2 percent since FFY 2007, compared with a 6.5 percent growth in total Medicaid spending.
- Compared with FFY 2022, Medicaid managed care spending as a percent of total Medicaid spending in FFY 2023 increased by 0.5 percentage points to 59.6 percent.
Table 1. Medicaid MCO Expenditures as a Percentage of Total Medicaid Expenditures, FFY 2007−2023 ($M)

As the table below indicates, 68.9 percent of FFY 2023 spending came from federal sources, which is 11.5 percentage points higher than the pre-Medicaid expansion share in FFY 2013 and 1.3 percentage points higher than FFY 2020.
Table 2. Federal versus State Share of Medicaid Expenditures, FFY 2013−2023 ($M)

State-Specific Growth Trends
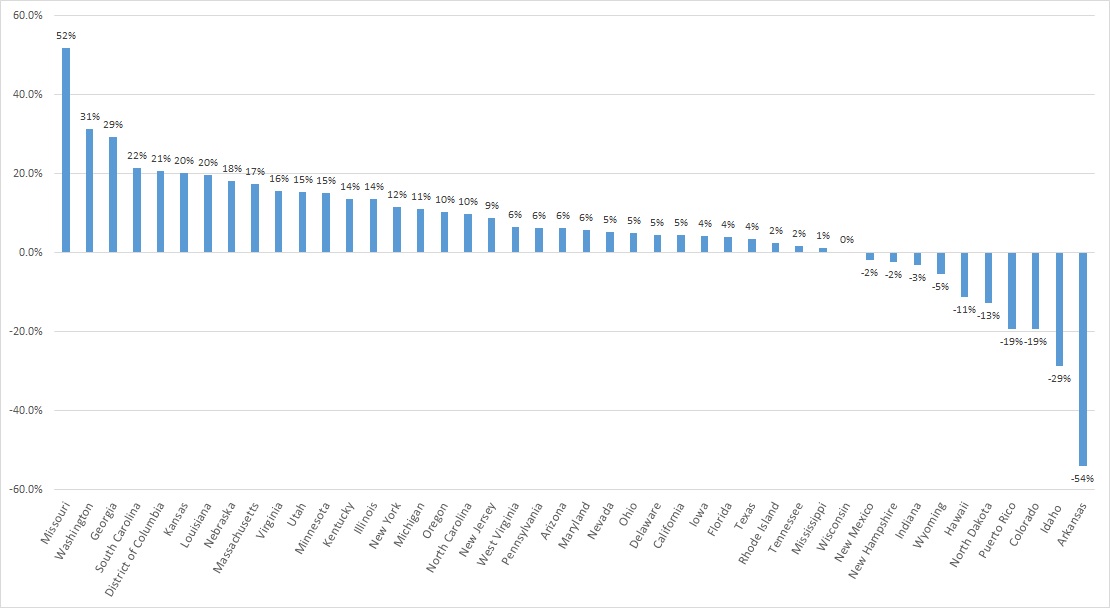
A total of 44 states and territories report managed care organization (MCO) spending in the CMS-64 report. Average MCO spending during FFY 2023 increased 8.5 percent. On a percentage basis, Missouri experienced the highest year-over-year growth in Medicaid managed care spending at 51.7 percent, followed by Washington at 31.4 percent and Georgia at 29.3 percent.
The chart below provides additional detail on Medicaid managed care spending growth in states with risk-based managed care programs in FFY 2023.
Figure 1. Medicaid Managed Care Spending Growth on a Percentage Basis by State, FFY 2022-2023
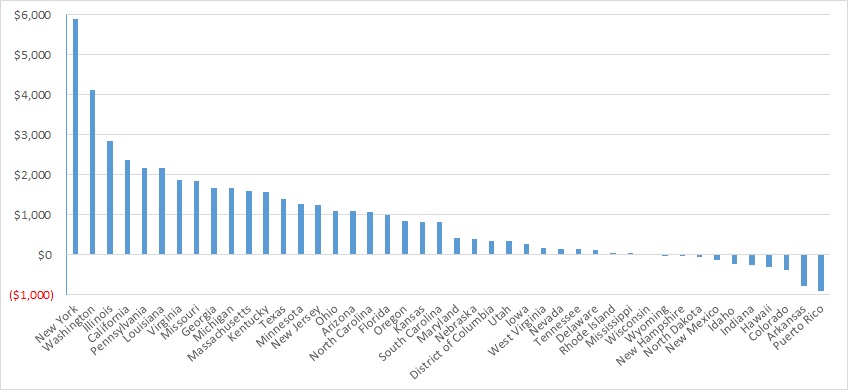
Looking at year-over-year spending growth in terms of dollars, New York experienced the largest increase in Medicaid managed care spending at $5.9 billion. Other states with significant year-over-year spending increases included Washington ($4.1 billion), Illinois ($2.8 billion), and California ($2.4 billion). The chart below illustrates the year-over-year change in spending across the states.
Figure 2. Medicaid Managed Care Spending Growth on a Dollar Basis by State, FFY 2022−2023 ($M)
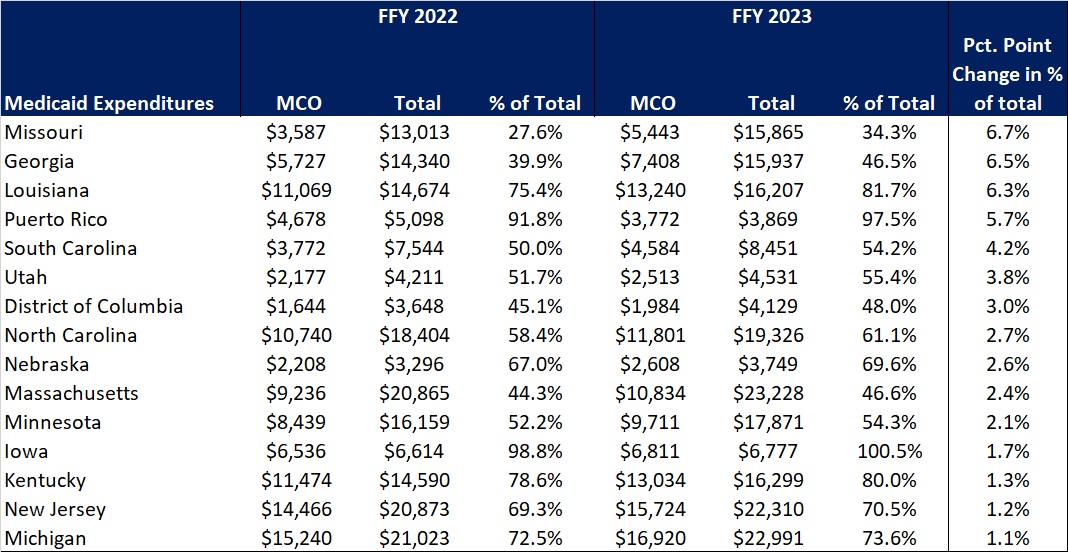
The percentage of Medicaid expenditures directed through risk-based Medicaid MCOs increased by more than one percentage point in 15 states from FFY 2022 to FFY 2023. The managed care spending penetration rate rose 6.7 percentage points in Missouri, 6.5 percentage points in Georgia, 6.3 percentage points in Louisiana, and 5.7 percentage points in Puerto Rico. In all, 22 states saw a decrease in managed care penetration from FFY 2022 to FFY 2023.
Table 3. Medicaid MCO Expenditures as a Percentage of Total Medicaid Expenditures in States with a One percent or Greater Increase from FFY 2022 to FFY 2023 ($M)
The table below ranks the states and territories by the percentage of total Medicaid spending through Medicaid MCOs. Iowa reported the highest percentage at 100 percent, followed by Puerto Rico at 97.5 percent and Kansas at 94.5 percent.
In many states, certain payment mechanisms may never be directed through managed care, such as supplemental funding sources for institutional providers and spending on retroactively eligible beneficiaries. As a result, the maximum achievable penetration rate in each state will vary and may be below the amount achieved in other states. The Medicaid managed care spending penetration rate is greatly influenced by the degree to which states have implemented managed long-term services and supports (MLTSS) programs.
Table 4. Medicaid MCO Expenditures as a Percent of Total Medicaid Expenditures, FFY 2016-2023
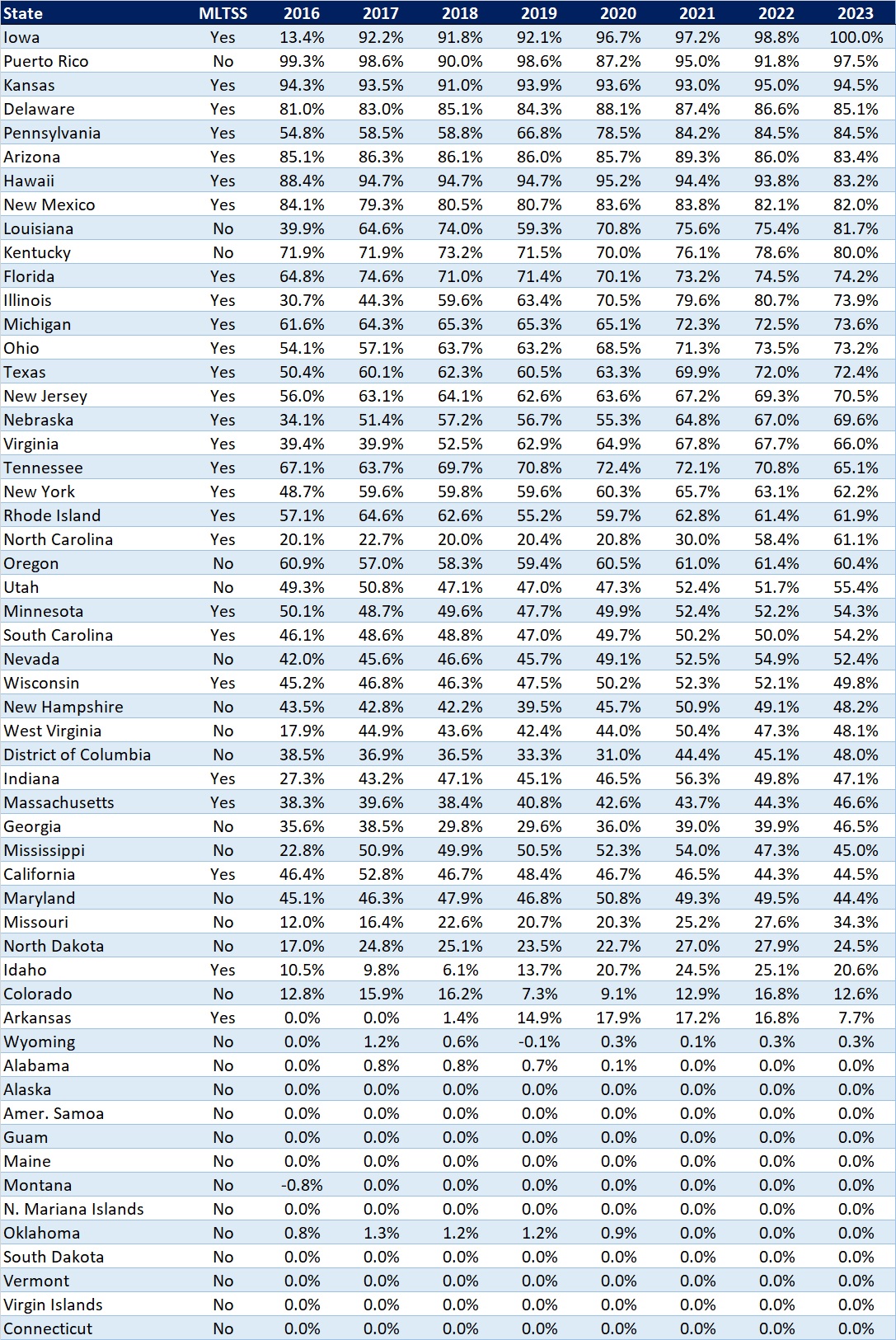
Note: Washington was excluded from the data table.
If you’re interested in becoming an HMAIS subscriber and for access to the CMS-64 data, contact Andrea Maresca at [email protected].
North Carolina releases foster care specialty plan program RFP
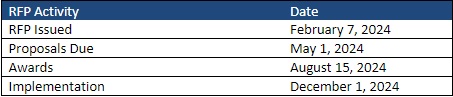
This week, our In Focus section reviews the statewide North Carolina request for proposals (RFP) for the new Children and Families Specialty Plan (CFSP), which the North Carolina Department of Health and Human Services (DHHS) released on February 7, 2024. The plan will provide physical health, behavioral health, intellectual and developmental disability, long-term care, and pharmacy services to children, youth, and families that the child welfare system serves. Implementation is scheduled for December 1.
Background
North Carolina implemented Medicaid managed care on July 1, 2021, after working on a plan to transition individuals from fee-for-service to managed care since 2015. CFSP is one of the four types of integrated Medicaid managed care plans the state will contract with to serve Medicaid beneficiaries. The other three are Standard Plans, the Behavioral Health and Intellectual/Developmental Disability (BH IDD) Tailored Plans, and the Eastern Band of Cherokee Indians Tribal Option.
Standard Plans are operated by one of two types of Medicaid managed care organizations (MCOs): statewide commercial plans (CPs) or regional provider-led entities (PLEs). The state awarded contracts to four CPs, the maximum allowed under the procurement, and one PLE. AmeriHealth Caritas North Carolina, Blue Cross and Blue Shield of North Carolina, UnitedHealthcare of North Carolina, and WellCare of North Carolina serve beneficiaries across six Medicaid managed care regions. A regional contract with provider-led Carolina Complete Health, a partnership between the North Carolina Medical Society and Centene, covers Regions 3, 4, and 5. The total value of the contracts is approximately $6.4 billion. The plans serve more than 2 million members as of year-end 2023.
The state plans to implement BH IDD Tailored Plans July 1. Tailored plans will be provided through the awarded local management entity-managed care organizations (LME-MCOs): Alliance Health, Partners Health Management, Trillium Health Resources, and Vaya Health. Implementation has been delayed multiple times since 2022. As a result, the state issued a directive last year to dissolve the Sandhills Center and consolidate Eastpointe and Trillium Health Resources to hasten the delayed rollout. The tailored plans are expected to cover approximately 160,000 beneficiaries.
Details about the CFSP
The following populations will be enrolled automatically in CFSP:
- Beneficiaries who are in foster care
- Beneficiaries who are receiving adoption assistance
- Beneficiaries enrolled in the former foster youth eligibility group
- The minor children of enrolled parents
The following populations will be eligible for enrollment in CFSP during contract year two:
- Parents, caretaker relatives, guardians and custodians with children in foster care
- Minor siblings of beneficiaries in foster care
- Adults identified on an open Child Protective Services (CPS) In-Home Family Services Agreement case and any minor children living in the same household
- Adults identified in an open Eastern Band of Cherokee Indians Department of Public Health and Human Services Family Safety program case and any children living in the same household
- Any other beneficiary that has been involved with the child welfare system who could benefit from enrollment
RFP
The state will award the contract to a single statewide managed care plan. Applicant MCOs will need to develop strategies for engaging with historically marginalized populations, addressing health disparities, and incorporating health equity. Technical proposals will be evaluated based on the following criteria:
- Medicaid Managed Care Qualifications and Experience
- Medicaid Managed Care Program Administration
- Administration and management
- Program operations
- Claims and encounter management
- Financial requirements
- Compliance
- Technical specifications
- Historically underutilized businesses
- Diversity, equity, and inclusion
- Integrated and Coordinated Delivery of Services
- Members and recipients
- Benefits and services
- Providers
- Stakeholder engagement
- Comprehensive Care Management
- Care management
- Quality and value
Timeline
The CFSP data book and capitation rate methodology will be released March 1, with an overview for presentation at a pre-proposal conference on March 7. Proposals are due May 1 and awards are expected to be announced August 15. Contracts are scheduled to run December 1, 2024, through June 30, 2028, with one additional option year. The RFP indicates that the Department will work with awardee to establish an appropriate launch date.
Driving change in healthcare delivery: HMA Spring Workshop builds towards policy and strategy frameworks necessary to implement value-based care
Federal policy frameworks establishing alternative payment models in Medicare and Medicaid have been the kick-starter of value-based care (VBC) innovation in healthcare delivery. However, employers provide health insurance to most Americans, and very few employers – with the exception of jumbo, self-insured employers – have leaned heavily into VBC. Small- and medium-sized firms rely on brokers to find an affordable health insurance plan, and often lack the resources required to negotiate more. Though the tide has been changing, our fragmented payment system has yielded only a subset voluntarily taking substantial risk for patient outcomes.
It has been said that to truly transform our American healthcare system to pay for value – improved outcomes for lower cost – it would require better alignment across public and commercial payers to support care providers in shifting their business models to take risk.
Quality and cost information are critical to implement VBC payment and delivery systems. Federal initiatives in Medicare and Medicaid have opened the door for providers, payers, and innovators to use health information to improve outcomes, with patients more engaged and more in control; the “Universal Foundation” announced by the Centers for Medicare and Medicaid Services (CMS) in 2023 seeks to align quality measures across the more than 20 CMS quality initiatives; and policies included in the 21st Century Cures Act and CMS Interoperability and Patient Access rule are creating more transparency on price and quality.
By enabling an infrastructure to measure, digitize, and share cost and quality information, federal and state governments have set the stage for greater collaboration among all purchasers – including employers – and the healthcare delivery system to redesign care that addresses health related social needs and behavioral health, ensuring that healthcare is provided equitably and sustainably. As the care delivery system is better able to deliver high value care, more employers will demand this for their workforce to provide a better benefit to their workers.
These issues, and more, will be a part of the expert-led conversation on VBC at HMA’s 2024 Spring Workshop March 5-6, in Chicago. This workshop offers a unique opportunity for payers, government officials, community organizations, vendors, and providers to have an unvarnished conversation about the challenges, lessons, and opportunities in implementing VBC. The meeting is designed to share insights, change-oriented strategies and actions that advance VBC from top industry experts, health plan executives, state and federal leaders, and policy experts.
Our working sessions will feature solutions-focused conversations among peers:
- Care delivery measures that drive outcomes, equity, population health
- Payment & risk management models for payment, pricing, attribution
- Data that is interoperable, consumer focused, deploying technology that is aligned to deliver on strategic objectives
- Policy & Strategy Frameworks at federal, state, and local levels that incentivize VBC
The closing panel will look at ways to take action through policy and collaboration to move our industry toward more sustainable approaches to healthcare payment and delivery.
To learn more and register for this unique event, please visit HMA’s 2024 Spring Workshop page. Act fast – online registration ends Wednesday, February 28!
Interoperability and patient access final rule: the next phase in the data exchange journey
This week, our In Focus section reviews the Centers for Medicare & Medicaid Services (CMS) Interoperability and Prior Authorization Final Rule, published on January 17, 2024. This is CMS’s latest effort to flesh out regulations mandating payer interoperability and fully electronic prior authorization (PA) policies. The 2024 final rule also represents a new phase in the agency’s work to advance interoperability as it moves beyond policymaking focused on building interoperable systems to policies centered on the applications and usage of shared data.
The new requirements affect a large segment of the nation’s public health insurance programs, including Medicare Advantage (MA) organizations, state Medicaid fee-for-service (FFS) programs, state Children’s Health Insurance Program (CHIP) FFS programs, Medicaid managed care plans, CHIP managed care organizations, and qualified health plan (QHP) issuers on the federally facilitated exchanges (FFEs). These payers must implement and adhere to Health Level 7® (HL7®) Fast Healthcare Interoperability Resources® (FHIR®) application programming interfaces (APIs). These APIs were developed by the DaVinci project and the CARIN Alliance which are both HL7 FHIR accelerator programs. Leavitt Partners, an HMA company, leads the work of the CARIN Alliance.
The final rule demonstrates a commitment to information sharing across the industry landscape and confidence in the FHIR standard to support health data exchange across all required APIs. Ultimately, FHIR APIs are creating a more patient-centered data ecosystem that can provide a tangible return on investment.
Following are details about the requirements, opportunities, and next steps for stakeholders.
Prior Authorization API and Process
Payers must build and maintain PA APIs by January 1, 2027, allowing providers to ask payers whether PA is required for a patient’s procedure, what documents must be submitted to attain authorization, and to receive the final decision and reason for denied requests electronically within a specified timeframe (seven days for standard procedures and three days for expedited decisions).
The rule finalizes requirements for the PA process, regardless of whether the payer receives the PA request through the Prior Authorization API. Specifically, CMS is requiring that:
- Affected payers send notices to providers when they make a prior authorization decision, including a specific reason for denial when they deny a PA request
- Payers, other than QHP issuers on the FFEs, respond to prior authorization requests within specific timeframes
- Affected payers publicly report certain metrics about their PA processes
These prior authorization process requirements become effective January 1, 2026. The last 12 months of PA information also must be shared with patient, providers, and other payers when the member switches a plan through the respective APIs.
To promote adoption of electronic prior authorization processes, CMS is adding an Electronic Prior Authorization measure for Medicare clinicians who participate in the Merit-based Incentive Payment System (MIPS) and hospitals and critical access hospitals in the Medicare Promoting Interoperability Program as an attestation measure.
Payer to Payer FHIR API
To support continuity of care and value-based programs, payers must be able to send, receive, and incorporate enrolled member data from previous and concurrent payers if members are dually enrolled.
To comply with the new electronic data sharing, the final rule requires payers to build and use FHIR API by January 1, 2027. Payer-to-payer (P2P) data sharing will include the last five years of claims/encounters, clinical data, and the active and pending PA requests. The data collected through the P2P APIs will need to be available to the other APIs (i.e., provider, patient, and prior authorization). The rule requires payers to request data from previous payers within a week after the patient opts in to sharing data. For dually enrolled members, data sharing will incur at least quarterly.
Patients must opt in and agree to the P2P data sharing. To this end, health plans must adjust their enrollment administrative process to allow members to easily share previous and concurrent payer information and consent to data sharing. CMS allows Medicaid or CHIP agencies to contract with entities, such as Health Information Exchanges (HIEs), for the digital access and transfer of a patient’s medical records, which supports the Payer-to-Payer API.
Provider Access FHIR API
Payers also must build and maintain a Provider Access API to share patient data with in-network providers with whom the patient has a treatment relationship, enabling continuity and coordination of care, by January 1, 2027. Affected payers must maintain an attribution process to associate patients with the appropriate in-network providers responsible for the patient care. The data from the payer via the Provider Access API must be added to a provider’s electronic health record, practice management solution, or any other technology solution that a provider uses for treatment purposes.
The Provider Access API includes the same data covered in the Payer to Payer Access API (claims/encounters, clinical data, and prior authorizations). The payer has one business day to deliver the required information. Payers must offer a mechanism for members to opt out from making their data available to the attributed providers.
Patient Access FHIR API
The final rule further enhances patient access to data to improve their treatment and shopping experience. In addition to claims and clinical data, as of January 1, 2027, payers must make PA data available through the Patient Access API to inform patients on their plan’s PA process and the status of requests.
In addition, affected payers must report annual metrics about Patient Access API usage and data requests to CMS beginning January 1, 2026.
Key Considerations and Early Results
The rule presents a significant opportunity to improve patient experiences and outcomes and to address some of the administrative burden on clinicians. Though CMS made some adjustments to timeframes in the proposed rule, immediate attention is needed to evaluate technological solutions available to payers, assess gaps between current and future required state, and develop policies to comply with new requirements and measures reporting.
Commercial payers may also leverage the improved electronic data sharing but are not required to do so. CMS-funded payers must respond to any inquiries from commercial payers and must require commercial payers to provide the same information as affected payers. Commercial payers, state governments, and other stakeholders have an opportunity to collaborate around the electronic data exchange.
This rule may have positive downstream application to other areas beyond PA, including quality measurements, risk adjustment, and population health. Early adopters who have implemented the prior authorization APIs have, on average, recorded a 150% – 300% return on investment (ROI). The implementation of API-based prior authorization represents a demonstrable increase in efficiency and significantly reduced provider burden. Given the measurable ROI, state-based regional collaboratives being led by Leavitt Partners are forming between payers and providers to implement the core tenants of the CMS rule well in advance of the 2027 deadline.
Similar initiatives are taking place in the technology space, like the Digital Quality Implementers Community, which was recently convened by Leavitt Partners and National Committee for Quality Assurance (NCQA) to build industry readiness for transitioning to FHIR-based digital measurement that hinges on improved electronic data sharing
What to Watch
The HMA team will continue to analyze the CMS’s Interoperability and Patient Access rule in the context of other federal and state policy changes affecting MA organizations, Medicaid FFS programs, state CHIP FFS programs, Medicaid and CHIP managed care programs, and QHPs.
The work and opportunities afforded with the Interoperability and Patient Access final rule will be featured prominently at The HMA Spring Workshop: Getting Real About Transforming Healthcare Quality and Value, March 5-6. In addition to rich discussions, HMA and HMA companies, including Leavitt Partners and Wakely Consulting LLC, are available to support planning and implementation and related system redesign initiatives. If you have questions about these topics, contact Ryan Howells ([email protected]) and Daniela Simpson ([email protected]).
Pennsylvania releases community HealthChoices (CHC) Medicaid managed care RFA
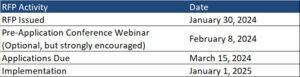
This In Focus section reviews the request for applications (RFA) that the Commonwealth of Pennsylvania Department of Human Services (DHS) released January 30, for the Community HealthChoices (CHC) Program. CHC is the mandatory managed long-term services and supports (MLTSS) program, which serves five CHC zones that cover all 67 counties in the commonwealth.
Notably, this procurement, as compared to the original CHC procurement in 2018, has increased emphasis on innovative approaches to address health equity and the Social Determinates of Health (SDOH). The health equity focus goes beyond traditional health-related social needs such as access to housing, transportation, food, and employment, and addresses some SDOHs that have a particular impact on the CHC population, such as environmental conditions and addressing hazardous or unsafe living conditions.
Behavioral health remains carved-out to separate behavioral health managed care organizations (BH-MCOs). Instead, CHC applicants will need to articulate how they will coordinate with the BH-MCOs to ensure access to appropriate BH services, which continues to be an area of significant interest for state Medicaid officials.
Background
The CHC Program serves individuals who are dually eligible for Medicare and Medicaid and people with physical disabilities who receive home and community-based waiver services or nursing facility care.
Participants may receive LTSS in the community or in a nursing facility.
CHC is the sole program option for fully dual eligible beneficiaries and most nursing facility clinically eligible (NFCE) individuals who reside in the five zones. The regional CHC zones are as follows:
- Southwest zone: Allegheny, Armstrong, Beaver, Bedford, Blair, Butler, Cambria, Fayette, Green, Indiana, Lawrence, Somerset, Washington, and Westmoreland counties.
- Southeast zone: Bucks, Chester, Delaware, Montgomery, and Philadelphia Counties.
- Remaining zones and respective counties, including
- Lehigh/Capital zone: Adams, Berks, Cumberland, Dauphin, Fulton, Franklin, Huntingdon, Lancaster, Lebanon, Lehigh, Northampton, Perry, York
- Northeast zone: Bradford, Carbon, Centre, Clinton, Columbia, Juniata, Lackawanna, Luzerne, Lycoming, Mifflin, Monroe, Montour, Northumberland, Pike, Schuylkill, Snyder, Sullivan, Susquehanna, Tioga, Union, Wayne, Wyoming.
- Northwest zone: Cameron, Clarion, Clearfield, Crawford, Elk, Erie, Forest, Jefferson, McKean, Mercer, Potter, Venango, Warren
RFA
Medicaid managed care organizations (MCOs) may submit applications for one or more zones. Applications are due March 15, 2024. The department anticipates awarding agreements to three to five CHC-MCOs in each of the five CHC zones. Selected applicants must provide CHC services in all counties in the zone(s) for which they are selected to participate and improve the accessibility, continuity, and quality of services for participants in the CHC program. The contract will run for five years and will have three one-year renewal options.
DHS indicates that the awarded CHC-MCOs must have an aligned dual-eligible special needs plan (D-SNP) and a current Medicare Improvement for Patients and Providers Act (MIPPA) agreement with the department. The aligned D-SNP must be operational and the MIPPA agreement must be in place by the anticipated implementation date (January 1, 2025).
DHS indicates selected MCOs must be as flexible and adaptable as possible and demonstrate the ability to coordinate services for multiple populations and across multiple programs, including programs with a focus that is broader than the delivery of healthcare services and LTSS.
Other RFA highlights include the following:
- Does not require a cost submittal.
- Includes small diverse business (SDB) or veteran business enterprise (VBE) goals of 11 percent and 3 percent respectively. Applicants must include separate SDB and VBE submittals for each zone in its application.
- Includes a contractor partnership program (CPP) which requires entities that are awarded a contract or agreement with DHS to establish a hiring target to support Temporary Assistance for Needy Families (TANF) beneficiaries in obtaining employment with the contractor, grantee, or their subcontractors.
Notably, DHS has provided itself flexibility within the RFA to implement a pay-for-performance incentive to MCOs. Under this policy, DHS could make incentives available to MCOs that help participants successfully complete the financial eligibility redetermination process with their local County Assistance Offices (CAOs). The department may implement additional pay-for-performance incentives in later years.
Timeline
Evaluation
For an applicant to be considered responsible for this RFA and eligible for selection of best and final offers (BAFOs) and negotiations:
- The total score for the technical submittal of the application must be greater than or equal to 75 percent of the available raw technical points
- The applicant’s financial information must demonstrate that the organization possesses the financial capacity to fulfill the good faith performance of the agreement
The evaluation committee will evaluate technical submittals for each zone separately. For each zone, DHS must select for negotiations the applicants with the highest overall score. The weight for the technical criterion is 100 percent of the total available points. Technical evaluation will be based on soundness of approach, applicant qualifications, personnel qualifications, and understanding the project.
The final technical scores will be determined by giving the maximum number of technical points available to the application with the highest raw technical score. The remaining applications will be rated by applying the formula located at RFP Scoring Formula.
Financial information will not be scored as part of the technical submittal. It will be reviewed only to determine an applicant’s financial responsibility.
SDB and VBE participation submittals will not be scored, however, if an applicant fails to satisfy the SDB or VBE requirements described, and DHS will reject the application.
DHS will not score the CPP submittal. Once an applicant has been selected for negotiations, DHS will review the CPP submittal.
Current Market
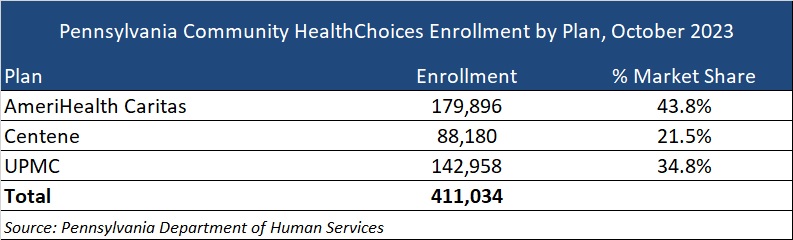
The CHC incumbents are AmeriHealth Caritas, Centene, and University of Pittsburgh Medical Center (UPMC), serving 411,034 CHC members as of October 2023.
DHS has published a historical data summary for the CHC program along with other DHS reports at: Community HealthChoices Historical Data.
Link to solicitation: All files on PA eMarketplace
Want to know more about how the next phase of Community Health Choices will impact your organization?
HMA’s Pennsylvania-based teams can assist organizations seeking to understand the implications of this important procurement, key program changes and what the outcome may mean for providers, community base organizations, and other stakeholders. Please contact Dianne Bisacky with questions or if you are seeking more detailed analysis of this procurement or the Community Health Choices program generally.
Nine States to Participate in Children’s Behavioral Health Policy Lab
LANSING, MICH. – Health Management Associates (HMA), in partnership with the Annie E. Casey Foundation, Casey Family Programs, National Association of State Mental Health Program Directors (NASMHPD), the Child Welfare League of America (CWLA), the American Public Human Services Association (APHSA), National Association of Medicaid Directors (NAMD) and the Centene Foundation, will convene a Children’s Behavioral Health (CBH) State Policy Lab, Feb. 7-9 in Baltimore. HMA today announced that Georgia, Kansas, Kentucky, Maryland, Missouri, Pennsylvania, Texas, Utah, and Wisconsin will participate in the policy lab. MITRE, which previously hosted a related federal convening, will also take part in this state convening.
This pioneering effort, made possible by the partner organizations, aims to convene state interagency teams – including child welfare, juvenile justice, behavioral health, Medicaid, and K-12 public education – to collectively strategize, learn from innovators in the sector and promote cross-system alignment to drive outcomes for children, youth, and families.
COVID-19 has exacerbated long-standing system collaboration challenges across state child welfare, behavioral health, and Medicaid that lead to unsatisfactory outcomes for the most vulnerable children in our communities. Most worrisome is the worsening of behavioral and physical health challenges and trauma because of uncoordinated or fragmented care. This lack of coordinated strategy and policy leads to higher costs of treatment and also increasingly exposes states and local jurisdictions to threats or filings of class action lawsuits, and related settlements or those arising from Department of Justice investigations. Fortunately, federal and state efforts and investments to address the youth systems of care – including schools, community, delivery systems, and community-based child placing agencies – are in motion.
In November, a call for applications was released to U.S. states and territories for potential participation in the State Policy Lab. Applicants were required to identify demonstrated need, existing state agency governance structures focused on children and youth, technical assistance needs, and outcomes for attending the policy lab. The applications required demonstrated participation from Medicaid, child welfare and behavioral health agencies; a commitment to creating sustainable interagency solutions for children, youth, and their families and had to certify formal support from the Governor/Cabinet level.
An external independent panel reviewed applications for state agency participation using a standardized rubric that covered four domains:
- Gaps and opportunities analysis
- Intent of collaborative partnerships
- Approach to engagement of youth and adults with lived experience
- Imminent risks to public agency operations as a result of poor outcomes for children, youth, and their families
This convening is aimed at assisting child welfare, juvenile justice, behavioral health, Medicaid, and K-12 public education where possible to build upon existing efforts to improve outcomes for children, youth, and families, strategically layering on missing components and promoting alignment between them and with other agency priorities. Examples of what could be co-designed with state partners:
- Build a shared strategic vision for a comprehensive continuum of care that ensures access to the “right service, at the right time based on individual and family need.” This vision can strengthen prevention initiatives and ensure the full array of evidence-based community-based interventions including use of crisis response and stabilization models.
- Develop policies and strategies for improving the engagement of children, youth, and families with lived experiences to the “right part of the system for the right level of care,” agnostic of the door through which they enter any coordinated child serving system, while ensuring that all aspects of this system are anchored in equity.
Following the event, learnings and findings will be disseminated to help states and counties adopt innovative solutions to improve outcomes for children, youth, and their families.
For more information email: [email protected]
CMS approves next phase of New York’s Medicaid 1115 waiver journey
This week, our In Focus section describes New York State’s Medicaid Section 1115 waiver amendment authorizing at least $6.7 billion in funding for new programs and initiatives in the state’s Medicaid program. The Centers for Medicare & Medicaid Services (CMS) approved New York’s application for the amendment January 9, 2024, which is effective retrospectively to April 1, 2022, through March 31, 2027.
New programs and initiatives are intended to improve access to services for Medicaid enrollees and include:
- Regional social care networks (SCNs) responsible for screening, referring, and providing new health-related social needs (HRSN) services to eligible Medicaid beneficiaries
- A statewide health equity regional organization (HERO), which will provide data analysis, regional needs planning, stakeholder engagement, value-based payment recommendations; and program analyses
- Workforce initiatives, including student loan repayment (SLR) and career pathways training (CPT) to recruit and retain healthcare professionals in high-need fields
- A Medicaid hospital global budget initiative (MHGBI) to provide funding to safety-net hospitals with negative operating margins to support their participation in waiver-related services
- An institution for mental diseases (IMD) waiver for substance use disorder (SUD) services
- A commitment from the states to sustain and enhance Medicaid provider payment rates to ensure access to services
Funding
CMS authorized at least $6.7 billion in funding. Some waiver components are without specific monetary valuation (i.e., IMD waiver, payment rate increases).
| DY 25 (ends 3/31/24) | DY 26 (ends 3/31/25) | DY 27 (ends 3/31/26) | DY 28 (ends 3/31/27) | Total | |
| HRSN Infrastructure | $0 | $260,000,000 | $190,000,000 | $50,000,000 | $500,000,000 |
| HRSN Services | $3,173,000,000 | ||||
| HERO | $50,000,000 | $40,000,000 | $35,000,000 | $125,000,000 | |
| Workforce: Student Loan Repayment | $12,080,000 | $24,150,000 | $12,080,000 | $48,310,000 | |
| Workforce: Career Pathways Training | $175,770,000 | $310,480,000 | $159,500,000 | $645,750,000 | |
| Medicaid Hospital Global Budget Initiative | $550,000,000 | $550,000,000 | $550,000,000 | $550,000,000 | $2,200,000,000 |
| $6,692,060,000 |
HRSN
- NY will implement 13 SCNs in nine regions, which are expected to establish networks of community-based organizations (CBOs) that provide HRSN services.
- Contracted SCNs, which will be awarded pursuant to a recently published request for applications, will receive infrastructure funding to invest in technology, business and/or operational practices, workforce development, and outreach and stakeholder engagement.
- SCNs will be reimbursed according to a state-published fee schedule for delivering HRSN services on a fee-for-service basis.
- SCNs are responsible for screening for HRSN and determining Medicaid beneficiaries’ eligibility level for enhanced HRSN services, spanning case management, nutrition supports, housing supports, and transportation.
HERO
- NY will contract with a single statewide Health Equity Regional Organization (HERO), which is independent of state or other government entities.
- The HERO will be responsible for five activities:
- Collect, aggregate, analyze, and report data
- Conduct regional needs assessments and planning
- Convene regional stakeholders
- Make recommendations to support advanced VBP arrangements and develop options for incorporating HRSN into VBP methodologies
- Conduct program analyses
Workforce
- The waiver approval identifies two pathways for workforce investment:
- SLR program for people who will serve in certain healthcare workforce shortage professions
- CPT program to support recruitment and advancement in healthcare careers
Medicaid Hospital Global Budget Initiative
- The MHGBI will be available to certain safety-net hospitals that meet governance, solvency, and geographic requirements.
- The MHGBI provides incentive payments to these hospitals if they:
- Collect and report data
- Meet milestones for transitioning to alternative payment models
- Demonstrate improvement in healthcare quality and equity
- As a condition of MHGBI, New York will apply for participation in the CMS Innovation Center’s AHEAD model.
IMD Waiver for SUD
- CMS approved an IMD waiver for SUD services. As a result, NY will be eligible to receive federal financial participation for Medicaid members who are short-term residents in IMDs for services that would not otherwise be matchable
- The state anticipates 50 providers will enroll within the first year
Curious About What the Waiver Means for Your Organization?
HMA’s New York Team can assist organizations assessing opportunities and understanding implications tied to these new, significant waiver investments. They have been working with key stakeholders to help inform the design of foundational components of the new wavier initiatives. HMA’s team of experts anticipate that the terms and conditions agreed to in the New York amendment provide important policy insight and direction for other states pursuing similar initiatives. Please contact Cara Henley and Josh Rubin with questions or if you are seeking more detailed analysis of the state’s waiver amendment.

Webinar replay – Navigating change: exploring the opportunities of New York’s 1115 Medicaid waiver amendment
This webinar was held on January 24, 2024.
During this webinar, HMA panel guides you through the newly approved key provisions of New York’s 1115 Medicaid waiver amendment. This groundbreaking development opens doors to transformative changes in healthcare delivery, impacting both providers and beneficiaries alike, including enhanced Health Related Social Needs (HRSN) benefits, workforce and hospital investments, and further commitment to Value Based Payment (VBP).
Gain valuable insights into the innovative strategies and opportunities presented by the waiver amendment, paving the way for new social care networking activities, funding opportunities, and regulatory flexibilities that will improve access to vital services.
This webinar shared information on waiver-specific details and what they mean, what potential opportunities will become available, and heard from national experts on similar models implemented nationally.