HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights – including our new podcast – puts the vast depth of HMA’s expertise at your fingertips, helping you stay informed about the latest healthcare trends and topics. Below, you can easily search based on your topic of interest to find useful information from our podcast, blogs, webinars, case studies, reports and more.
Health Management Associates (HMA) has partnered with the National Association of State Mental Health Program Directors (NASMHPD) Technical Assistance Coalition to produce a series of briefs that characterize the opportunities to improve coordination of services for children.
The significance of caregiver support for healthy early childhood outcomes is highlighted in this brief “Early Childhood Mental Health: The Importance of Caregiver Support in Promoting Healthy Child Development and Clinical Interventions for Children written by HMA experts Christina Altmayer, Caitlin Thomas-Henkel and Uma Ahluwalia. This brief explores the role of Medicaid in advancing early childhood child mental health outcomes, the importance of caregiver support in promoting healthy child development, and innovative practices aimed at increasing access to supports.
Health Management Associates (HMA) has partnered with the National Association of State Mental Health Program Directors (NASMHPD) Technical Assistance Coalition to produce a series of briefs that characterize the opportunities to improve coordination of services for children.
Connecting Schools to the Larger Youth Behavioral Health System: Early Innovations from California focuses on the role schools can play in ensuring that children and youth get the behavioral healthcare they need. Written by HMA experts, Michael Butler, Ilia Rolon, Caitlin Thomas-Henkel and Uma Ahluwalia, this brief outlines California’s innovative approach to expanding access while describing the lessons learned and potential implications for other states.
Health Management Associates (HMA) offered a 3-part series of webinars looking at the effect of proposed regulations on delivery of opioid treatment services to the population facing addiction issues. In this third and final webinar, HMA consultants highlighted opportunities for state regulators to shape policy and regulation of substance use disorder (SUD) treatment.
New federal regulations encourage significant changes to how opioid treatment is provided, with the goal of expanding access and improving patient-centered care. State regulators will need to adapt their regulatory practices and work closely with Medicaid agencies and treatment providers so the new regulations can achieve their intended goals. This webinar discussed how State Opioid Treatment Authorities (SOTAs), licensing entities, and state Medicaid agencies will need to work together to craft updated regulations, facility licensing, and reimbursement practices that advance person-centered care.
HMA experts were joined by Allegra Schorr, VP, West Midtown Medical Group and President of the Coalition of Medication-Assisted Treatment Providers and Advocates (COMPA). COMPA represents New York State’s Opioid Treatment Programs (OTPs), as well as providers offering office-based medication-assisted treatment, currently providing addiction treatment to over 43,000 New Yorkers.
Learning Objectives:
New Regulatory Requirements – Overview of state rules around opioid treatment vs the new requirements.
How to Improve SUD Treatment Access – Specific recommendations on statutory and regulatory changes that could lead to more patient centered treatment options.
States Leading the Way – Examples from states that are leading the way to expand access and reduce stigma.
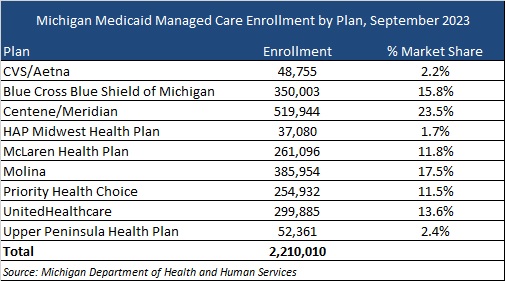
This week, our In Focus section reviews the Michigan Medicaid Managed Care Comprehensive Health Care Program (CHCP) request for proposals (RFP), which the Michigan Department of Health and Human Services released on October 30, 2023. CHCP covers 2.2 million Medicaid members and is worth approximately $15 billion.
MIHealthyLife
The rebid is part of MIHealthyLife, an initiative that the department launched in 2022 to strengthen Medicaid services through new Medicaid health plan contracts. At that time, Michigan Medicaid sought input from nearly 10,000 stakeholders in an effort to strengthen Medicaid managed care contracts and create a more equitable, coordinated, and person-centered system of care. Based on the feedback, the department designed the RFP with a focus on five strategic pillars:
• Serve the Whole Person, Coordinating Health and Health-Related Needs • Give All Kids a Healthy Start • Promote Health Equity and Reduce Racial and Ethnic Disparities • Drive Innovation and Operational Excellence • Engage Members, Families and Communities
RFP
Medicaid managed care organizations (MCOs) serve 10 regions, each consisting of multiple counties. MCOs will bid on one or more of the regions throughout the state. Each region requires at least two plans, with the exception of Region 1, a rural area that includes Michigan’s Upper Peninsula, where members are enrolled in a single plan.
As part of the MIHealthyLife initiative, the RFP will include the following changes:
• Prioritizing health equity by requiring Medicaid health plans to achieve National Committee for Quality Assurance Health Equity Accreditation • Addressing social determinants of health through investment in and engagement with community-based organizations • Increasing childhood immunization rates, including greater provider participation in the Vaccines for Children program • Adopting a more person-centered approach to mental health coverage • Ensuring access to health care providers by strengthening network requirements • Increasing Medicaid Health Plan accountability and clarifying expectations to advance state priorities
Timeline
Proposals are due January 16, 2024, and implementation is anticipated to begin October 1, 2024. Contracts will run through September 30, 2029, with three one-year optional periods.
Current Market
Michigan currently has nine plans, which serve more than 2.2 million Medicaid and expansion members. The table below provides a breakdown of the plan market share by enrollment.
This week, our In Focus section summarizes the Medicaid Long-Term Services and Supports (LTSS) Annual Expenditures Report, which the Centers for Medicare & Medicaid Services (CMS) released on October 17, 2023. The report includes detailed information about Medicaid LTSS expenditures for federal fiscal year (FY) 2020, which runs from October 1, 2019, through September 30, 2020. During this time, LTSS spending grew 20 percent to $199.4 billion from the previous year.
Medicaid LTSS Expenditures
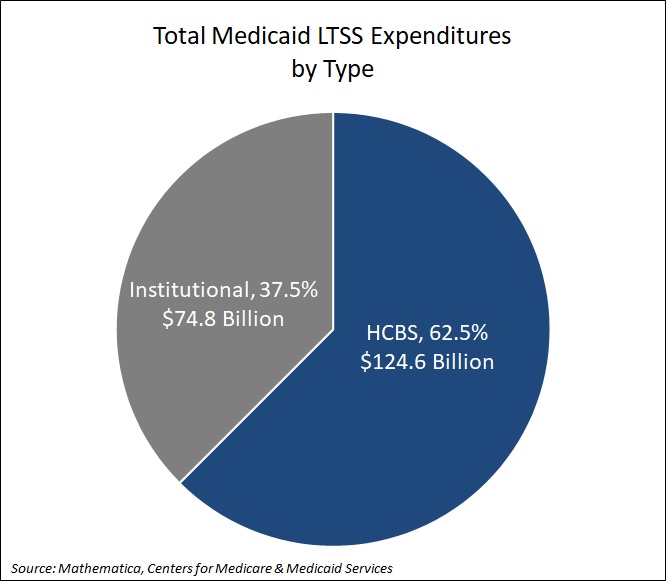
Medicaid LTSS expenditures cover home and community-based services (HCBS), which includes personal care and home health, as well as institutional care, which includes services provided in nursing facilities, intermediate care facilities (ICF) for individuals with intellectual or developmental disabilities (IDD), and mental health facilities. HCBS accounted for 62.5 percent ($124.6 billion) of LTSS expenditures. The remaining 37.5 percent, or $74.8 billion, was directed toward institutional care (see Figure 1).
Figure 1. Medicaid LTSS Expenditures by Type
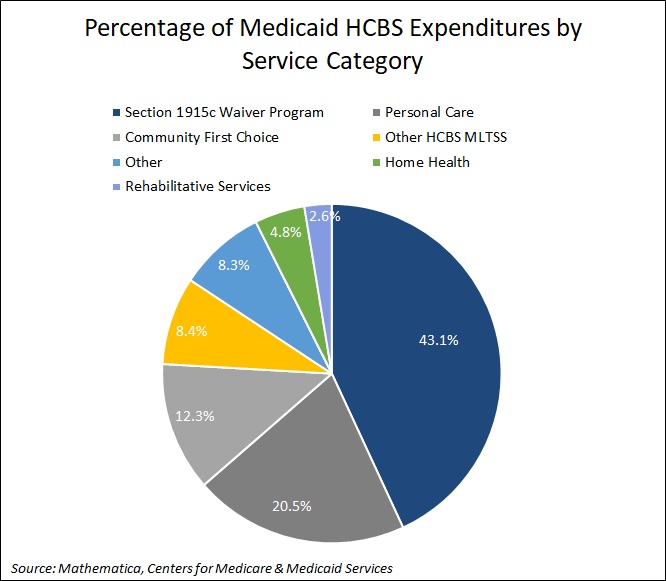
In addition, Section 1915c waiver program spending accounted for 43.1 percent of HCBS expenditures, followed by personal care at 20.5 percent. See Figure 2 for additional breakouts.
Figure 2. Percentage of Medicaid HCBS Expenditures by Service Category
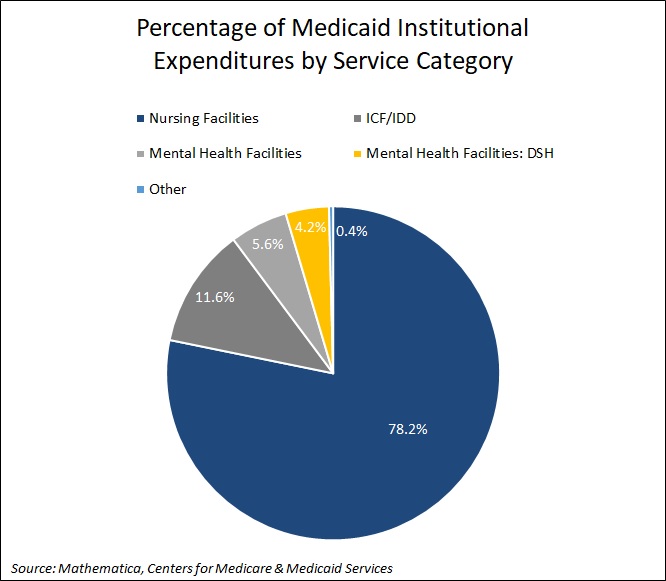
Nursing facilities accounted for the largest percentage (78.2 percent) of institutional care spending. See Figure 3 for additional breakouts.
Figure 3. Percentage of Medicaid Institutional Expenditures by Service Category
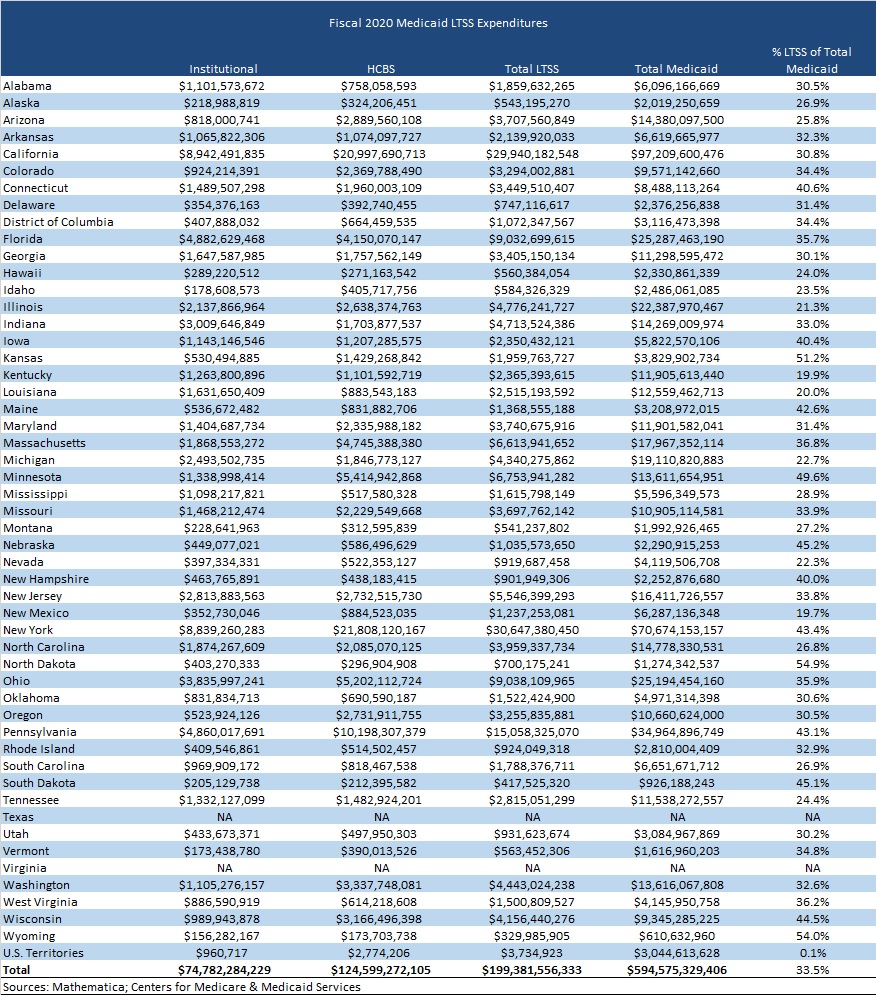
Medicaid LTSS spending accounted for 33.5 percent of total Medicaid spending in FY 2020. States with the highest LTSS as a percentage of total Medicaid spending were North Dakota at 54.9 percent, Wyoming at 54 percent, Kansas at 51.2 percent, Minnesota at 49.6 percent, and Nebraska at 45.2 percent. Texas and Virginia did not report spending for Medicaid LTSS programs, which comprise a substantial share of total LTSS expenditures in those two states (see Table 1).
Table 1. Medicaid LTSS Expenditures by State
LTSS spending per resident also varied from state to state. On average, states spent $679 Medicaid LTSS dollars per state resident in FY 2020. Utah had the lowest Medicaid LTSS expenditures per state resident at $284, whereas the District of Columbia had the highest at $1,554 per resident.
Medicaid MLTSS Expenditures
Medicaid managed long-term services and supports (MLTSS) spending totaled $57 billion in FY 2020. HCBS accounted for $35.7 billion and institutional care accounted for $21.3 billion. As more states adopted and extended their Medicaid managed care programs, MLTSS spending grew 750 percent from FY 2008.
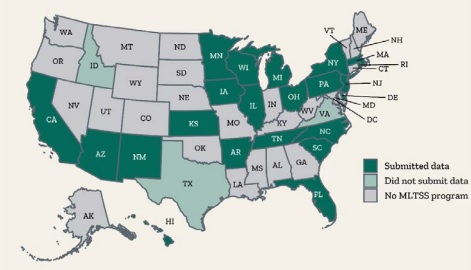
In FY 2020, 25 states had operational MLTSS programs. Of these, nine were Financial Alignment Initiative (FAI) capitated model demonstrations for dual eligible members. New York, Pennsylvania, Florida, and California accounted for 58 percent of total MLTSS spending nationally, with New York representing 23 percent of total national MLTSS expenditures. Three states—Idaho, Texas, and Virginia—did not report MLTSS spending (see Figure 4).
Figure 4. States with MLTSS programs, FY 2020
Source: Mathematica
Iowa had the highest share of MLTSS expenditures as a percentage of total Medicaid LTSS expenses in FY 2020 at 95 percent. Arizona and Kansas followed at 94 percent and Hawaii at 74 percent. The national average was 29 percent. At the lowest end were South Carolina at 4 percent and Rhode Island at 12 percent, both of which are fee-for-service states. Michigan followed at 14 percent.
Contributing Factors to LTSS Expenditures
The COVID-19 public health emergency, which includes the first six months of the pandemic that started in March 2020, had a major effect on LTSS expenditures in FY 2020. Many residents in long term care facilities are covered by Medicaid and disproportionately experienced the most COVID-19 deaths. States began to implement various policies to address the impact of COVID-19 among Medicaid LTSS users. This includes modifying utilization limits for covered services and increasing payment rates for certain institutional services and HCBS.
As mentioned earlier, Texas and Virginia did not report Medicaid LTSS expenditures, which undercut the national total. Other factors that affect the reliability of Medicaid LTSS data include changes in state MLTSS expenditure reporting methods, and changes in state Medicaid LTSS policies and programs.
Note: CMS hired Mathematica to conduct the research, which used CMS-64 Medicaid expenditure report data, state-reported MLTSS data, Money Follows the Person (MFP) worksheets for proposed budgets, CMS 372 data on section 1915(c) waiver program population groups, and U.S. Census data to compile the report
Public schools face persistent pressure to serve as the central point for addressing children’s overall health and well-being. Behavioral health and access to care challenges were a growing concern affecting school populations even before the Covid pandemic.
Youth are experiencing behavioral health crises at an alarming rate, and schools are struggling with insufficient resources for students to receive the necessary person-centered care and support. Sustainable funding streams, including options like Medicaid and alternate funding methods, could help schools effectively cover expenses. New temporary funding streams are available (e.g., CMS School Based Health Services Program, Bipartisan Safer Communities Act, and multiple state funding initiatives) but schools often lack the necessary infrastructure, administrative support, and awareness of community resources to effectively utilize these funds.
Our Clients
HMA works with state and local education agencies, school districts, county offices of education, departments of public instruction, social service agencies, public health, school boards, and family and parent organizations to support school-based mental health initiatives.
Through innovations in community partnerships, evidence-based programming, and design that support healthy children and promising futures, there is opportunity to enhance school outcomes. Students’ well-being and mental health directly impact their overall educational experience and achievement. By addressing these challenges and investing in comprehensive BH support within schools, we can help schools design an environment that furthers the well-being and success of all students.
HMA can help school systems:
Add capacity for project management support for whole-child approaches to improved health
Reduce duplication of services
Assess opportunities to better leverage new and existing resources and dollars through blended and braided funding and existing community-based supports to enhance utilization
Strengthen infrastructure and awareness and establish collaborations and partnerships to ensure effective utilization of available funding and shared resources
Break down bureaucratic silos and promote interagency cooperation
Improve information and data sharing
Emphasize preventative behavioral and physical care
Assess strategies for workforce shortages
Develop and implement evidence-based integrated care clinics within schools
Deliver training for administration, staff, parents, and community partners that helps achieve successful adoption
Implement targeted initiatives to address ongoing and pervasive stigma surrounding behavioral health, particularly in specific cultures and communities
HMA has the right team
With our expertise and collaborative approach, we empower schools and school districts to proactively address the youth behavioral health crisis and create a supportive educational environment for all students.
Our team members have extensive careers in school-based mental health, direct clinical behavioral health practice, healthcare systems, as well as government social services and public health, community organizations, and school-based leadership. Our experts have worked with every type of stakeholder, gaining invaluable insights and understanding. We meet schools where they are and help to right-size service offerings. HMA can bring a fresh perspective on school-based services, and help you shift from reactive to proactive.
Along with a comprehensive understanding of the behavioral healthcare continuum, Annalisa Baker’s experience includes business operations, project management, finance, and … Read more
During his career, Michael Butler has directed hundreds of program evaluation, organizational development, and technical assistance projects in a wide … Read more
Trish Marsik has extensive experience supporting providers, healthcare organizations, and state and federal governments to provide quality behavioral healthcare. Prior … Read more
This week, our In Focus section highlights a white paper that Wakely, a Health Management Associates company, released in October 2023, “Cut to the Point: A Summary of 2024 Star Rating Cut Point Changes”. The paper reviews 2024 Medicare Star Rating data, including the Star Rating Technical Notes, which the Centers for Medicare & Medicaid Services (CMS) released October 13, 2023.
The data summarizes how Medicare Advantage Organizations (MAOs) performed on various quality measures during the 2022 measurement year and serves as an indication of changing Medicare Advantage spending in 2025 as a result of changes in Medicare Advantage Prescription Drug (MA-PD) Overall Star Ratings. The publication of the 2024 Star Rating Technical Notes provided an opportunity for Wakely to analyze measure-level cut point changes. This paper looks at the latest cut point changes to determine how the Tukey Outlier Deletion methodology and changes in the overall quality performance have affected Star Rating cut points.
Wakely will also host a webinar, Stars and Strikes: 2024 Star Ratings and the Impact of Tukey, at 2:30 pm ET on November 14, 2023. The webinar will cover the recently released 2024 Star Ratings, including an analysis of the expected impact on 2025 Medicare payments. Attendees should expect to hear discussions about the latest program changes and resulting impact on the contract-level star ratings, including implementation of the Tukey outlier deletion methodology. In addition, Wakely colleagues will cover the upcoming changes to the Star Rating program and discuss their potential impact on Medicare Advantage Organizations.
For questions, please contact our Wakely experts below.
Lifting Voices is an initiative developed to inform the transformation of the youth behavioral health care system. The project leaders are parents of children who nearly died on multiple occasions from severe behavioral health conditions, and they are professionals with a deep understanding of the opportunities and challenges faced by behavioral health care policy makers and reformers. They share the belief that their knowledge, desperation, and resources afforded their children access to interventions that should be accessible to every youth who needs them. Their experience of the care delivery system has also inspired their commitment to highlight the urgent improvements necessary to support struggling children and parents affected by the nation’s youth behavioral health crisis.
To learn more about Lifting Voices, see the October 2023 report here.
HMA Principals and behavioral health policy and practice transformation consultants Heidi Arthur, LMSW and Ellen Breslin, MPP partnered with Sheilah Gauch, LISW, M.Ed., Principal and Clinical Director with the Dearborn Academy and Echo Lustig, B.A., young adult behavioral health advocate, to share findings from the first phase of the three-part Lifting Voices initiative at Putting Care at the Center, the annual conference of the Camden Coalition’s National Center for Complex Health and Social Needs Initiative. See: Putting Care at the Center 2023, Elevating behavioral health in whole-person care. Boston, MA, November 1-3, 2023. Please look for us at the Beehive poster station on: