HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights – including our new podcast – puts the vast depth of HMA’s expertise at your fingertips, helping you stay informed about the latest healthcare trends and topics. Below, you can easily search based on your topic of interest to find useful information from our podcast, blogs, webinars, case studies, reports and more.
This article was the latest in the Health Affairs Forefront series, Medicare and Medicaid Integration which features analysis, proposals, and commentary that inform policies on the state and federal levels to advance integrated care for those dually eligible for Medicare and Medicaid.
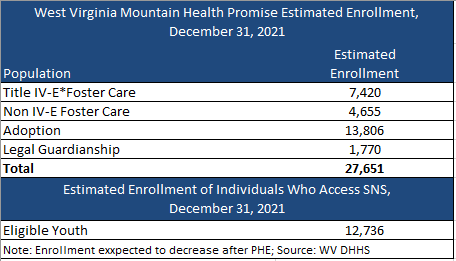
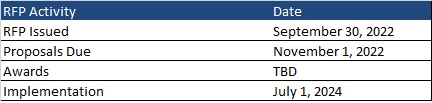
This week, our In Focus section reviews the Mountain Health Promise request for proposals (RFP) released by the West Virginia Department of Health and Human Resources on September 30, 2022, for specialized Medicaid managed care for children and youth in foster care.
Mountain Health Promise RFP
The selected managed care organization (MCO) will provide physical and behavioral health services to children and youth in the foster care system, individuals receiving adoption assistance, youth formerly in foster care up to age 26 who aged out of foster care while on Medicaid in the state of West Virginia, and children eligible under the children with serious emotional disorders (CSED) waiver. Potential expansions could include, but are not limited to, children at risk for foster care placement and the family of youth in crisis. Additionally, the MCO will act as an administrative services organization (ASO) and provide statewide administrative services for all individuals accessing socially necessary services (SNS).
Some of the goals of the program include:
Enhance coordination and access to services
Enhance quality of care and minimize barriers for youth and families/improve access to treatment
Reduce fragmentation and offer seamless continuity of care
Improve health and social outcomes for youth and impacts on families
Help reduce the number of children removed from the home and reduce lengths of stay per episode of care through increased family-centered care that provides necessary and coordinated services to all members of the family
Decrease children involved with the juvenile justice and corrections systems
Reduce out-of-home and out-of-state placements
Develop new or enhance existing services, such as children’s mobile crisis response (CMCR), inState Psychiatric Residential Treatment Facilities (PRTF) to reduce the need for out-of-state placements, and intensive home-based treatment
Physical and behavioral health services will be reimbursed through a Medicaid per member per month (PMPM) capitation payment. For SNS administration, the Bureau for Social Services (BSS) will provide a fixed monthly rate. The PMPM capitation rate will not include carved out SNS costs.
It is encouraged, but not required, that the MCO subcontract with regional child welfare organizations, residential mental health treatment facilities (RMHTFs), and organizations that provide home and community-based services for children with serious emotional disorders to assist in the care coordination of services for this population.
Market
There are nearly 28,000 individuals currently enrolled in Mountain Health Promise, with about 13,000 eligible for SNS. Enrollment, however, is expected to decrease following the end of the Public Health Emergency (PHE). CVS Health/Aetna is the incumbent plan. Aetna had contracted with Kepro to serve as the ASO for SNS.
Timeline
Proposals are due November 1, 2022. The contract is anticipated to run from July 1, 2024, through June 30, 2025, with three one-year options.
Evaluation
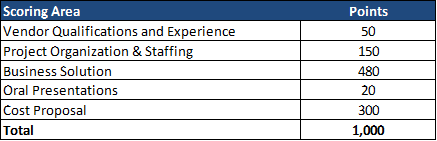
The winning MCO will be chosen based on the highest score of a possible total 1,000 points. The technical evaluation will be a total of 700 of 1,000 points. Cost represents 300 of 1,000 total points.
This week, our In Focus explores a new trend to watch in Medicaid Section 1115 waiver demonstration programs. As discussed in our previous In Focus, state Medicaid agencies are exploring pathways and concepts to address the historic inequities and health disparities laid bare and exacerbated by the COVID-19 pandemic. These efforts are closely aligned with the Centers for Medicare and Medicaid Services’ (CMS) policy objectives for the Medicaid program, specifically:
Addressing health inequities
Improving access and coverage
Promoting whole person care
Teams of experts from across the HMA family of companies are supporting state agencies, counties, health plans, providers, community and consumer organizations, and other stakeholders with translating federal goals and parameters into concrete proposals for new demonstration programs. HMA’s experts assist stakeholders with proposals as they move through the stages of concept paper, application, negotiation, approval, and implementation. Demonstrations will reflect each state’s unique political and policy landscapes, but the programs will be grounded in certain federal goals and expectations to enhance accountability and improve outcomes.
In the earlierIn Focus, our experts shared initial insights and considerations for stakeholders about one of the emerging trends: state Medicaid leaders are seeking to improve health equity in communities by providing health-related social services and engaging community organizations. Building on this and informed by our collective “on the ground” expertise we are writing this week about a second emerging trend we see across states’ Section 1115 activities:
Trend #2: States are seeking to use Medicaid demonstration programs to build essential capacity and infrastructure at the community and organizational levels.
The recently approved and submitted demonstration proposals signal CMS’ willingness to allow states to support some limited capacity building for community-based organizations. Several state 1115 demonstration proposals describe the state-specific types of community-based organizations and other entities that Medicaid programs want to engage to address the social and health-related drivers of health outcomes. This requires augmenting the existing workforce, providing training on Medicaid health plan contracting requirements, and building an infrastructure platform and systems that will support efficient communications and service delivery.
CMS has indicated a strong interest in advancing states’ community-based activities. This is evident in CMS’ decision to revise the federal framework used to determine whether a state’s Section 1115 demonstration program is budget neutral for the federal government. CMS has also decided to reopen the opportunity for states to propose Designated State Health Programs (DSHPs) under more limited size and scope parameters. CMS articulated these updated policies in the recent approval letters for Section 1115 demonstration programs in Massachusetts and Oregon. The federal reinterpretation provides states significantly more flexibility relative to the prior policy to use federal Medicaid funding to do the following:
Design and implement a broader set of health-related service need (HRSN) initiatives,
Make investments in the infrastructure to support HRSNs; and
Invest in building workforce capacity.
States will continue to act on these shifts in federal priorities and policies, crafting proposals aligned with their state-specific environments and goals. However, CMS’ willingness to support capacity building as part of state demonstration programs will need to adhere to certain scope and financing parameters. These guardrails are articulated in more detail in the approval letters for Massachusetts and Oregon. States and stakeholders will also want to be responsive to CMS’ expectations that its investments will be sustainable over time. They may need to plan and develop additional capacity to utilize non-Medicaid sources of federal and non-federal funding in tandem with the demonstration initiatives.
Importantly, the terms of the approved demonstration projects reinforce the need for states, managed care plans, and providers engage in new partnerships with community leaders and ensure the perspectives and experiences of consumers are continuously reflected in programs. Examples of proposed capacity building partnerships include:
Massachusetts’ recently secured CMS approval for a Section 1115 demonstration program which will fund a variety of health-related service needs (HRSN) initiatives. As part of the HRSN initiatives, CMS is allowing the state to receive federal Medicaid funding to support capacity-building, infrastructure, and operational costs for these activities. For example, under the demonstration federal funding will be available for participating “community partners” to pay for health information technology system investments, expand workforce capacity, manage startup costs, and enhance operational infrastructure such as system change resources. Additionally, the state will be able to receive federal Medicaid funding for provider workforce recruitment and retention activities, specifically primary care and behavioral health provider student loan repayment programs and a family nurse practitioner residency program.
In September 2022, Oregon received approval for a Section 1115 demonstration program to provide increased coverage of certain services that address HRSN. These services include critical nutritional services and nutrition education, as well as transitional housing supports for individuals with a clinical need or transitioning out of institutional care, congregate settings, out of homelessness or a homeless shelter, or the child welfare system. Additionally, the state will be able to receive federal Medicaid funding to make infrastructure investments to support those services, such as cultural competency training, trauma-informed training, traditional health worker certification, accounting and billing systems among others.
New York State envisions that Social Determinant of Health Networks (SDHNs) will work to organize and coordinate small neighborhood organizations familiar with their communities’ needs and the capacity to address multiple social risk factors as well as larger county or regionally focused entities. The state aims to allow SDHNs to receive Medicaid funding to invest in developing the infrastructure they need to assist Medicaid enrollees, such as the IT and business processes and other capabilities. Alongside this, the state is proposing a minimum fee schedule for certain services addressing social care needs. In addition, New York is requesting support for a statewide social services referral technology platform.
Washington state has a proposal pending with CMS that builds on its earlier demonstration program to further invest in multi-sector, community-based partnerships and approaches using Accountable Communities of Health (ACH). Specifically, the state is proposing to invest in the development and operation of Community Hubs and a Native Hub, which will serve as centers for community-based care coordination. These hubs will focus on health-related social needs (HRSNs) that provide screening for and referral to community-based services for Medicaid enrollees. These hubs will also distribute funding to build capacity among community-based organizations (CBOs) and community-based providers.
New Jersey has designed an 1115 demonstration proposal focused on the lack of stable housing as a driver of unnecessary hospitalization, institutionalization, or other avoidable instances of high-cost care, negative clinical outcomes, and worsening of chronic conditions. While it does not plan to make direct investments in community-based entities, the state aims to enhance contractual requirements with its Medicaid managed care organizations around housing specialists. This includes requiring health plans to have their housing specialists coordinate with community-based organizations that provide housing services or other related services to address social drivers of health. Its proposal also is designed to facilitate coordination across state and community resources that are essential to the provision of health and housing services.
Conclusion
The Massachusetts and Oregon demonstration programs provide important insight on CMS’ willingness to support state investments in HRSN and the state and local infrastructure to support delivery of culturally appropriate services.
Stakeholders will want to monitor these and other proposals as they move forward, particularly to understand the conditions and timing for funding to flow to community entities. Additionally, each state demonstration will have reporting and accountability structures that could impact payment and future investments made by Medicaid health plans, providers, CBOs and other stakeholders.
HMA’s interdisciplinary teams of Medicaid, human services, and actuarial experts are assisting states as well as stakeholders as they conceptualize, develop, and implement Section 1115 programs. To learn more about our work, contact our expert below.
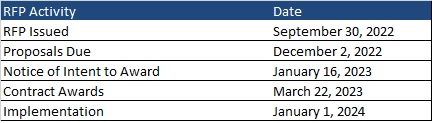
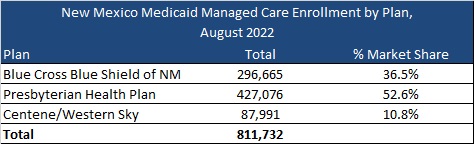
This week, our In Focus reviews the New Mexico Medicaid managed care request for proposals (RFP), released on September 30, 2022, by the New Mexico Human Services Department (HSD). The state will transition to a new program called Turquoise Care in 2024, which will build upon the current Centennial Care 2.0 program through a new Section 1115 waiver demonstration. Managed care organizations (MCOs) will provide physical health, behavioral health, and long-term care (LTC) services to approximately 800,000 Medicaid managed care members.
RFP
New Mexico plans to award Turquoise Care contracts to three MCOs. One of the selected MCOs will also be awarded a specialized foster care plan contract to provide services to Children in State Custody (CISC) on a statewide basis. CISC will be mandatorily enrolled and Native American CISC members will have the option to voluntarily enroll.
Turquoise Care will introduce new practices aimed at improving quality based on population health outcomes. The program will focus on three goals:
Goal 1: Build a New Mexico health care delivery system where every Medicaid member has a dedicated health care team that is accessible for both preventive and emergency care that supports the whole person – their physical, behavioral, and social drivers of health.
Goal 2: Strengthen the New Mexico health care delivery system through the expansion and implementation of innovative payment reforms and value-based initiatives.
Goal 3: Identify groups that have been historically and intentionally disenfranchised and address health disparities through strategic program changes to enable an equitable chance at living healthy lives. The target populations will be:
Prenatal, postpartum, and members parenting children, including children in state custody
Seniors and members with long-term services and supports (LTSS) needs
Members with behavioral health conditions
Native American members
Justice-involved individuals
Other changes for Turquoise Care include:
90 percent Medical Loss Ratio (MLR) aimed at improving quality of care
Expanded MCO reporting and monetary penalties for non-compliance
Minimum reimbursement rate for contract providers at or above the state plan approved fee schedule
More stringent provider network requirements
A single centralized vendor to process applications
Enhanced MCO staffing requirements, including qualifications, staffing levels, and training
Focus on social determinants of health
New Mexico will submit the Section 1115 demonstration waiver for Turquoise Health to the Centers for Medicare & Medicaid Services (CMS) for approval by December 2022. HSD will update the model contract to reflect the requirements related to the waiver renewal upon its approval.
During this procurement, the state will also be developing and implementing a new Medicaid Management Information System (MMIS).
Eligibility
Approximately 83 percent of the Medicaid population is in managed care.
Populations exempt from mandatory managed care enrollment are:
Native American members not in need of LTC
Individuals with Intellectual Disabilities (ICF-IID) in Intermediate Care Facilities
Individuals enrolled in Qualified Medicare Beneficiary (QMB), Specified Low-Income Medicare Beneficiary (SLIMB), or Qualified Individuals program
Individuals covered only under the Medicaid Family Planning program
Individuals enrolled in the Program of All-Inclusive Care for the Elderly (PACE)
Individuals covered pursuant to Emergency Medical Services for Non-Citizens (EMSNC)
Members in the Developmental Disabilities 1915(c) Waiver and in the Medically Fragile 1915(c) Waiver will continue to receive home and community-based services (HCBS) through that waiver but are required to enroll with an MCO for all non-HCBS.
Timeline
Proposals are due December 2, 2022. Contracts will run from January 1, 2024, through December 31, 2026, with optional one-year renewals, not to exceed eight years total.
Current Market
New Mexico had 811,732 Medicaid managed care as of August 2022, served by Blue Cross Blue Shield of New Mexico, Presbyterian Health Plan, and Centene/Western Sky. The state also had an additional 163,361 fee-for-service members.
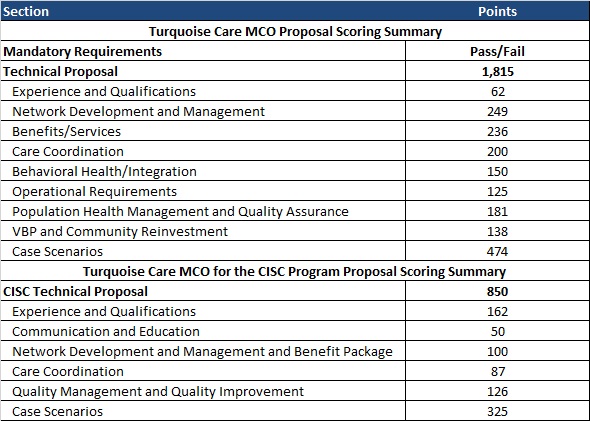
Evaluation
The evaluation process will consist of three phases: review of mandatory requirements, review and scoring of the technical proposals, and review and scoring of the CISC technical proposals.
This week, our In Focus section looks at the current federal policy landscape and trends and the legislative outlook for the remainder of 2022 and beyond. Experts from HMA continue to monitor developments in this area and provide additional updates as more information becomes available.
Legislative Branch
To date in 2022, Congress passed multiple comprehensive bills, including the Inflation Reduction Act (IRA), which was signed by President Biden on August 16, 2022. The IRA extends Exchange plan premium tax subsidies through 2025, institutes an out-of-pocket drug spending cap for Medicare beneficiaries, expands Medicare, Medicaid, and CHIP coverage protections for certain vaccines, allows Medicare to negotiate drug prices, and implements a penalty payment in the Medicare program for prescription drug prices that rise faster than the rate of inflation.
Going forward, stakeholders have an extensive list of immediate Medicare payment issues for Congress to tackle while lawmakers continue to consider fundamental reforms to the program. Priorities include mitigating Medicare payment reductions scheduled for 2023; providing relief to address inflationary cost pressures; extending the 5 percent bonus for physicians participating in Advanced Alternative Payment Models (APMs), which expires at the end of 2022 for Accountable Care Organizations (ACOs); and permanently expanding telehealth access and payment policies after the federal COVID-19 public health emergency (PHE) declaration expires. Many stakeholder groups are also urging the Senate to act on the House-approved legislation, Improving Seniors Timely Access to Care Act (H.R. 3173), to reform Medicare Advantage prior authorization policies.
Congress did not include major Medicaid proposals in the Inflation Reduction Act. Medicaid stakeholders want Congress to revisit certain Medicaid policies in one of the remaining legislative vehicles this year. Significant proposals of interest include closing the Medicaid coverage gap in non-expansion states, enhanced coverage for justice involved populations, and expanding support for home and community-based services (HCBS). States and some stakeholders have also sought more certainty in the timing and guardrails for ending the COVID-19 Public Health Emergency (PHE) policy that links enhanced federal Medicaid funding with the requirement for continuous Medicaid coverage.
Congressional leaders and key influencers are laying the groundwork for 2023 legislative efforts. Congress is likely to defer action on most major legislative issues until after the November mid-terms, including finalizing federal fiscal year 2023 funding for most departments. A change in control of either or both chambers of Congress will likely lead to greater scrutiny of the Biden Administration’s health care policies and actions, which have largely gone untested by this Congress.
Executive Branch
Executive orders have been a major source in driving federal workstreams in 2022. Following enactment of several major bills, implementation responsibilities have shifted to the Executive Branch and stakeholders will have multiple opportunities to further shape and support new programs, regulatory and policy updates, and funding opportunities. Executive orders passed include:
Advancing Racial Equity and Support for Underserved Communities, January 21, 2021
Promoting Competition in the American Economy, July 9, 2021
Improving the Customer Experience, December 13, 2021
Access to Affordable, Quality Health Coverage, April 5, 2022
Equality for LGBTQI Individuals, June 15, 2022
Protecting Access to Reproductive Healthcare Services, July 8, 2022
The Administration will continue to address COVID-19 emergency needs while stepping up efforts to support states, health plans, providers and other stakeholders as they prepare for the post-COVID environment. The current PHE declaration expires October 13, 2022, but since HHS has not signaled that it plans to end the PHE in October, another extension is likely until January 11, 2023. The next advance notification about the end of the PHE would be Nov. 12, 2022. Once the PHE declaration expires, numerous Medicare and Medicaid, TANF, and SNAP flexibilities will end, including Medicaid’s continuous coverage requirement and certain telehealth flexibilities, among others. Additional federal agency guidance is expected to support post-PHE transitions.
The Centers for Medicare & Medicaid Services (CMS) plans to advance new policy direction across several service and delivery areas, including strengthening long-term services and support and innovations via Section 1115 demonstration programs. CMS is expected to approve transformational 1115 proposals in additional states. Several state proposals focus, in part, on building capacity among local and regional entities and community-based organizations to address social drivers of health. Many state proposals are also strengthening behavioral health delivery systems and seek to meet enrollees’ urgent behavioral health needs. Additionally will want to monitor CMS’ regulatory efforts to align and strengthen managed care and fee-for-service (FFS) access and network adequacy policies as well as updates to the agency’s in lieu of services policy in managed care programs.
The Administration is also expected to accelerate work on its top policy priorities and regulatory agenda in advance of the next Presidential election, and this will require ongoing engagement among health care stakeholders.
For additional information on these and other policies, contact our experts below.
This week, our In Focus highlights a Health Management Associates Institute on Addiction (HMA IOA) report, Delaware Substance Use Disorder Treatment System Needs Assessment, published in June 2022. HMA IOA conducted a statewide three-county substance use disorder (SUD) treatment system needs assessment in Delaware. This project began in November 2021 and was primarily funded by New Castle County with contributions from Kent and Sussex counties. The goal was to review the current state of the SUD treatment ecosystem, identify strengths and gaps collecting input from as many Delawareans across multiple sectors as possible, and make actionable recommendations to build a more robust and sustainable future state system.
The final analysis included interviews with key stakeholders, focus groups, a survey of all licensed SUD providers, claims data analysis, and a comparison of Delaware’s public (e.g., Medicaid) outpatient and residential SUD reimbursement rates with selected regional states. This approach provided a unique cross-sector view of where the most significant opportunities for improvement and investment may rest.
The areas of greatest experienced need in the system were reported as: inadequate treatment beds, especially for some populations, like children and youth; lack of residential services for adults, especially those on Medicare and without insurance; needed supports for those experiencing negative impacts from social determinants of health (SDOH), like transportation and housing needs; lack of consistent access and care coordination; lack of adequate reimbursement to sustain the system or expand the treatment system; the need for trauma-informed care (TIC); and the need for more harm reduction and prevention strategies, including greater access specifically to Narcan 4mg Nasal Spray or its generic equivalent.
The study found that Delaware is meeting only 15 percent of SUD treatment needs and only meeting five percent of the need for the highest-intensity services, including inpatient treatment.
The results also showed an apparent discrepancy between what the state is working hard to implement to address the SUD and overdose crisis in Delaware and the community’s perception of, or lived experience with, those SUD treatment services and supports. Additionally, HMA IOA heard about many treatment system strengths from interviewees, town hall participants, and focus groups and included recommendations that are meant to leverage those existing strengths in the future treatment system.
On August 18, 2022, the Centers for Medicare and Medicaid Services (CMS) released a roadmap to support healthcare providers with preparing for the eventual end of the COVID-19 public health emergency (PHE) declaration. CMS also published a series of fact sheets summarizing the status of Medicare Blanket waivers and flexibilities by provider type as well as flexibilities applicable to the Medicaid providers and stakeholders.
In its announcement, CMS expressed concern that the continued PHE flexibilities could contribute to further decline in patient, resident, and client safety beyond what has already been observed. As a result, the agency is cautiously working to balance ongoing PHE needs while conveying more urgency for providers to prepare for the eventual end of the PHE flexibilities and waivers.
CMS has already ended certain flexibilities and waivers. The agency could phase out other flexibilities as it prepares to let the PHE declaration lapse. This means that providers and health plans should act now to assess flexibilities and waivers in use and develop a plan to transition to post-PHE environment.
Phase-out of COVID-19 Flexibilities
During the COVID-19 PHE, CMS has utilized Medicare and Medicaid waivers and flexibilities extensively. For example, Medicare has not enforced certain federal requirements during this time to allow hospitals to utilize off-site locations to screen and treat patients when needed as well as to minimize certain reporting requirements. The agency’s flexibilities also have accelerated adoption of telehealth and audio only services, particularly for behavioral health services.
Medicare and Medicaid providers across the states utilized PHE flexibilities to varying degrees, in part depending on experiences in individual communities, capacity, and other provider specific factors. Additionally, over the course of the PHE health plan and provider staffing and workflows have changed dramatically. This means health plans and providers will need a tailored plan to support the transition to the post PHE environment.
HMA’s experts are working with hospitals, health systems, clinics, and other providers as well as health plans on the steps they need to take now to prepare for multiple transitions. Our experts identified six immediate steps that Medicare and Medicaid plans and providers can be undertaking now to ensure they can effectively return to normal operations, including:
Review performance on the patient and clinician safety metrics cited in the new CMS resources. In instances where providers have gaps and suboptimal safety and quality outcomes they will need assistance developing and implementing mitigation and quality improvement plans.
Utilize CMS’ tailored fact sheets to identify specific flexibilities and waivers in use now and the “normal” federal regulations that will be in effect once the PHE lapses. This assessment should include the blanket waivers and provider specific flexibilities, including:
Flexibilities around the requirements and timing for practitioner training
Expansion of allowable sites of service that permitted more expansive use of telehealth and virtual services as well as screening and treatment provided at alternative sites
Relaxation of federal requirements pertaining to surge capacity protocols
Flexibilities for staffing requirements, including medical records departments, nursing facilities, among others
Waiver of requirement for hospitals to submit occupational mix surveys and to have a utilization review plan with a UR committee focused on services furnished to Medicare and Medicaid enrollees
Applicable of the Extreme and Uncontrollable Circumstances Policy in Medicare’s Shared Savings Program and use of other flexibilities for MSSP Accountable Care Organizations (ACOs)
Non enforcement of certain physician self-referral laws
Waiver of numerous reporting requirements including those pertaining to verbal orders, discharge planning, HEDIS and STARs measure reporting, among others
Project impact of ending Medicaid’s continuous coverage policy and support individuals with actions they may need to take at the end of the PHE. Once the PHE ends, Medicaid’s enhanced federal funding for states and continuous coverage policy will end. HMA is working with health plans, providers and other stakeholders to project how this change will impact the enrollment and payer mix on state and local levels. Additionally, patients and their caregivers will need support from plans, providers, and consumer groups to ensure they renew their coverage or transition to other coverage programs when needed. HMA’s experts have written extensively about our work to support the Medicaid unwinding activities in two blog posts – The PHE is continuing—what’s next for Medicaid? and How stakeholders can prepare now for unwinding of Medicaid public health emergency continuous eligibility.
Develop a plan to transition from “PHE” to “post-PHE” expectations that is informed by the assessment of flexibilities in use. Key components of the plan include:
Anticipated resource needs to reflect changes in staffing and workflows during the PHE
Articulation of specific compliance procedures and regular reporting requirements that will resume and the process for this transition
Develop training and education opportunities for staff that may be new or need refresher on normal policies and procedures as well as timeframes for making these changes
Update budgets projections to account for changes in reimbursement rates for certain services post-PHE. Certain reimbursement amounts and payment methodologies will change post-PHE, such as payment for administering the COVID-19 vaccine in a Medicare patient’s home among other changes. Providers will need to project the financial impact of these payment changes and update coding and billing manuals and procedures where applicable.
Build strategies to sustain changes to care models implemented during the COVID-19 PHE while also addressing health disparities. Some providers and facilities adopted care models and modified existing ones during the PHE that may have improved patient outcomes and experiences, maximized expertise of practitioners, and improved value-based care. For example, some providers have embraced the Medicare Hospital Without Walls Initiative and will need to assess their options as some of those flexibilities are phased out. Other federal opportunities have newly emerged during the pandemic, such as the Rural Emergency Hospital designation and pending changes to the Medicare Shared Savings Program (MSSP).
What’s Next
The COVID-19 PHE declaration next expires on October 12, 2022. While a renewal of the PHE declaration is possible into early 2023, providers should be using this time to prepare for resumption of normal policies and procedures.
The expiration of PHE flexibilities and waivers are not, however, happening in a vacuum. Providers need to make this transition amidst a dynamic healthcare sector with high expectations for continuous improvement in quality, patient experiences, and value. During this transitional period HMA’s experts are working with health plans and providers to develop or revisit strategic plans and investments to refocus attention on improving models of care and value-based payment approaches, including strategies that will help mitigate health disparities.
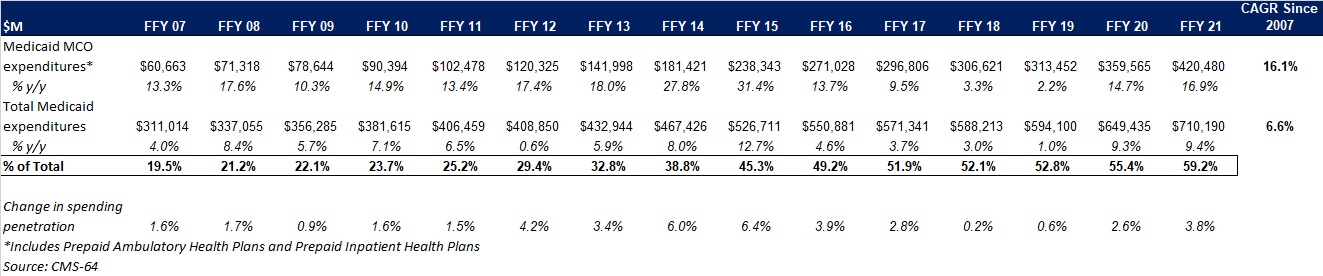
This week, our In Focus section reviews preliminary 2021 Medicaid spending data collected in the annual CMS-64 Medicaid expenditure report. After submitting a Freedom of Information Act request to the Centers for Medicare & Medicaid Services (CMS), HMA received a draft version of the CMS-64 report that is based on preliminary estimates of Medicaid spending by state for federal fiscal year (FFY) 2021. Based on the preliminary estimates, Medicaid expenditures on medical services across all 50 states and six territories in FFY 2021 was nearly $710.2 billion, with over 59 percent of the total now flowing through Medicaid managed care programs. In addition, total Medicaid spending on administrative services was $30.8 billion, bringing total program expenditures to $741 billion.
Total Medicaid Managed Care Spending
Total Medicaid managed care spending (including the federal and state share) in FFY 2021 across all 50 states and six territories was $420.5 billion, up from $359.6 billion in FFY 2020. This figure includes spending on comprehensive risk-based managed care programs as well as prepaid inpatient health plans (PIHPs) and prepaid ambulatory health plans (PAHPs). PIHPs and PAHPs refer to prepaid health plans that provide only certain services, such as dental services or behavioral health care. Fee-based programs such as primary care case management (PCCM) models are not counted in this total. Below we highlight some key observations:
Total Medicaid managed care spending grew 16.9 percent in FFY 2021. The rate of growth has been increasing since the COVID-19 pandemic. Prior to 2020, the rate had decelerated since FFY 2016.
Managed care spending growth was due in large part to the COVID-19 pandemic and the resulting higher Medicaid enrollment.
In terms of dollars, the increase in Medicaid managed care spending from FFY 2020 to FFY 2021 was $60.9 billion, compared to $46.1 billion from FFY 2019 to FFY 2020.
Medicaid managed care spending has increased at a compounded annual growth rate (CAGR) of 16.1 percent since FFY 2007, compared to a 6.6 percent growth in total Medicaid spending.
Compared to FFY 2020, Medicaid managed care spending as a percent of total Medicaid spending in FFY 2021 increased by 3.8 percentage points to 59.2 percent.
Figure 1: Medicaid MCO Expenditures as a Percentage of Total Medicaid Expenditures FFY 2007-2021 ($M)
As the table below indicates, 69.4 percent of FFY 2021 spending came from federal sources, which is 12 percentage points higher than the pre-Medicaid expansion share in FFY 2013, and 1.8 percentage points higher than FFY 2020.
Figure 2: Federal vs. States Share of Medicaid Expenditures, FFY 2013-2021 ($M)
State-specific Growth Trends
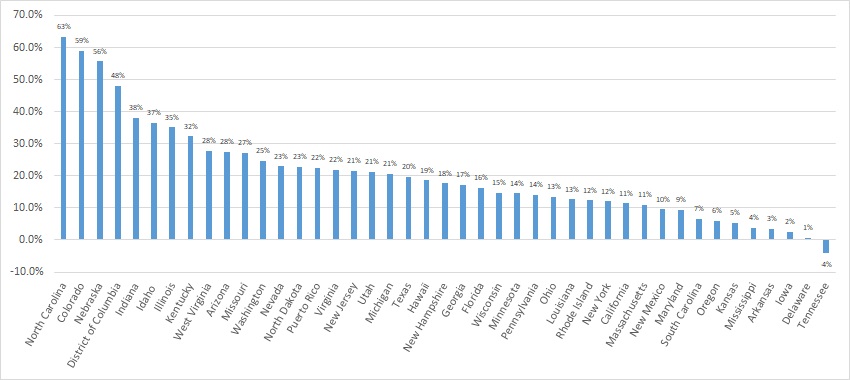
Forty-five states and territories report managed care organization (MCO) spending on the CMS-64 report, including Alaska, which utilizes a PIHP/PAHP model exclusively. Oklahoma is expected to implement a Medicaid managed care program in 2023. Of the remaining 44 states and territories that contract with risk-based MCOs, average MCO spending in FFY 2021 increased 17.6 percent. On a percentage basis, North Carolina experienced the highest year-over-year growth in Medicaid managed care spending at 63.3 percent due to the implementation of its risk-based Medicaid managed care program. Among states with more mature programs, Colorado experienced the fastest growth in FFY 2021 at 59 percent, followed by Nebraska at 55.6 percent.
The chart below provides additional detail on Medicaid managed care spending growth in states with risk-based managed care programs in FFY 2021.
Figure 3: Medicaid Managed Care Spending Growth on a Percentage Basis by State FFY 2020-21
Source: CMS-64; *Note: Not all states are included in the table.
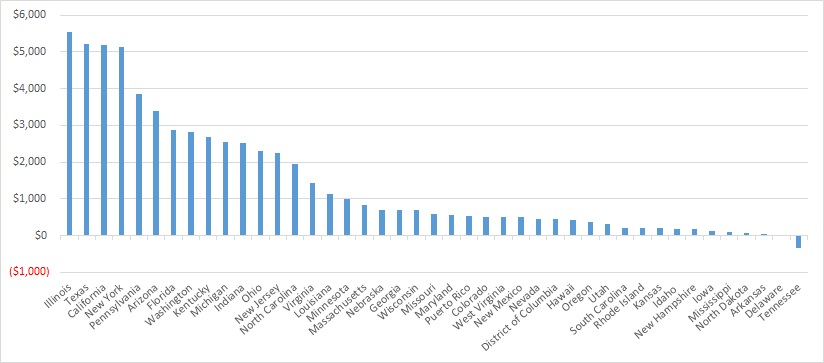
Looking at year-over-year spending growth in dollar terms, Illinois experienced the largest increase in Medicaid managed care spending at $5.5 billion. Other states with significant year-over-year spending increases in dollar terms included Texas ($5.2 billion), California ($5.2 billion), and New York ($5.1 billion). The chart below illustrates the year over year change in spending across the states.
Figure 4: Medicaid Managed Care Spending Growth on a Dollar Basis by State FFY 2020-21 ($M)
Source: CMS-64; *Note: Not all states are included in the table.
The percentage of Medicaid expenditures directed through risk-based Medicaid MCOs increased by more than five percentage points in 14 states from FFY 2020 to FFY 2021. The managed care spending penetration rate rose 13.4 percentage points in the District of Columbia, 9.7 percentage points in Indiana, 9.5 percentage points in Nebraska, 9.2 percentage points in North Carolina, and 9.1 percentage points in Illinois.
Figure 5: Medicaid MCO Expenditures as a Percentage of Total Medicaid Expenditures in States with a 5 percent or Greater Increase from FFY 2020 to FFY 2021 ($M)
Source: CMS-64
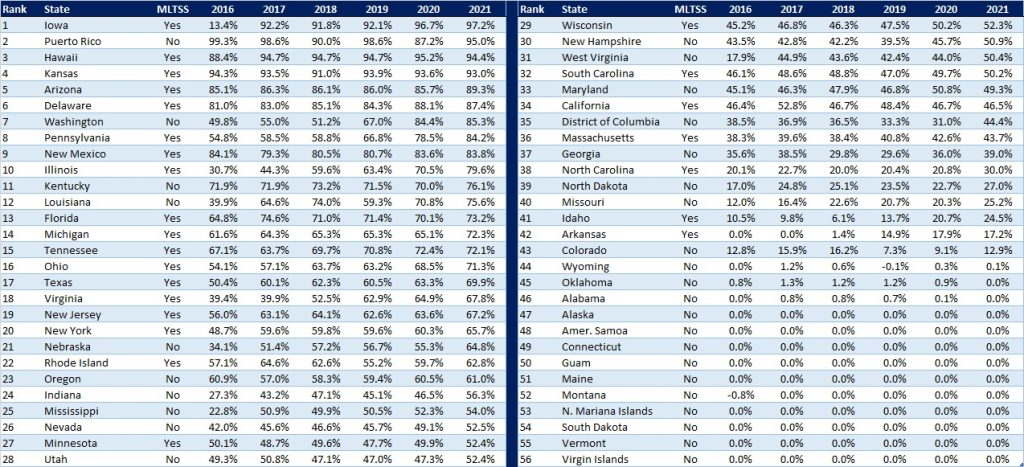
The table below ranks the states and territories by the percentage of total Medicaid spending through Medicaid MCOs. Iowa reported the highest percentage at 97.2 percent, followed by Puerto Rico at 95 percent, and Hawaii at 94.4 percent.
We note that in many states, there are certain payment mechanisms which may never be directed through managed care, such as supplemental funding sources for institutional providers and spending on retroactively eligible beneficiaries. As a result, the maximum achievable penetration rate in each state will vary and may be below that achieved in other states. The Medicaid managed care spending penetration rate is greatly influenced by the degree to which states have implemented managed long-term services and supports (MLTSS) programs.
Figure 6: Medicaid MCO Expenditures as a Percent of Total Medicaid Expenditures, FFY 2016-2021
Non-MCO Expenditures
Despite the rapid growth in Medicaid managed care over the last 10 years, program spending still represented approximately 59 percent of total Medicaid expenditures in FFY 2021. So where is the remaining fee-for-service (FFS) spending (approximately $291 billion) going? First, as noted above, there are many states/territories with Medicaid managed care programs in which certain beneficiaries or services are carved-out of the program, and these are typically associated with high-cost populations. The total amount of non-MCO spending in the 44 states with risk-based managed care in FFY 2021 was $260.4 billion. Assuming an average “full penetration” of 85 percent of total Medicaid spending, then HMA estimates that an additional $221 billion in current FFS spending could shift to a managed care model just in the states that already employ managed care for a subset of services and/or beneficiaries.
Thirteen states/territories did not utilize a comprehensive risk-based managed care model in FFY 2020. In general, the 13 states/territories that do not utilize managed care today are smaller states. Oklahoma, with $5.3 billion in Medicaid spending is expected to shift to risk-based Medicaid managed care in 2023. Total Medicaid spending across all 13 non-managed care states/territories was $29.8 billion. The 13 states/territories that did not employ a risk-based comprehensive Medicaid managed care model in FFY 2021 were Alabama, Alaska, American Samoa, Connecticut, Guam, Maine, Montana, Northern Mariana Islands, Oklahoma, South Dakota, Vermont, Virgin Islands, and Wyoming.
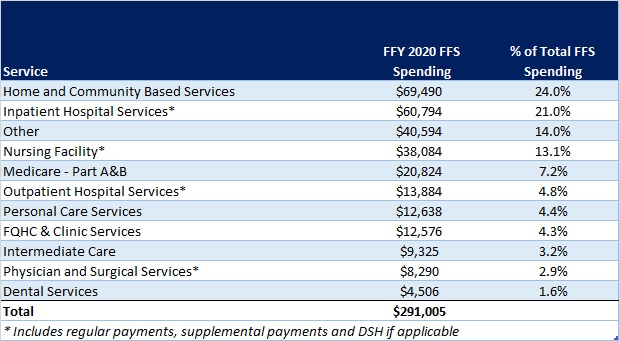
In terms of spending by service line, the largest remaining FFS category is home and community-based services at $69.5 billion, which accounts for 24 percent of FFS spending. Inpatient hospital services represent 21 percent of FFS spending at $60.8 billion.
Figure 7: Fee-for-Service Medicaid Expenditures by Service Line, FFY 2021
While the CMS-64 report provides valuable detail by service line for all FFS expenditures, it does not capture how spending directed to Medicaid MCOs is allocated by category of service. Therefore, it is not possible to calculate total MCO spending by service line, a challenge that will only intensify as more spending runs through MCOs.
This week, our In Focus section highlights an HMA Issue Brief, Bolstering the Youth Behavioral Health System: Innovative State Policies to Address Access & Parity, published in August 2022. The brief examines policies aiming to advance access and availability of behavioral health services (encompassing mental health and substance use disorders) for youth. Below we explore opportunities for states to adopt levers to ensure access to the full continuum of children’s behavioral health services. States should consider developing a multi-faceted strategy to address accessibility issues including:
A policy mechanism for insurance coverage and funding for infrastructure, support and services across behavioral health, child welfare and Medicaid
A robust delivery system for provision of services
Comprehensive benefit design
A mechanism to monitor network adequacy, access, and parity
The COVID-19 pandemic has exacerbated rates of depression, anxiety, and other behavioral health issues among youth – with suicide now the second leading cause of death among ages 10-12. Pre-pandemic, 1 in 5 children experienced a mental health condition every year and only 54 percent of non-institutionalized youth enrolled in Medicaid or CHIP received mental health treatment. Between March 2020 to October 2020, mental health–related emergency department visits increased 24 percent among youth ages 5 to 11 and 31 percent among ages 12 to 17, compared with 2019 emergency department visits.
Youth covered by Medicaid and the State Children’s Health Insurance Program (CHIP), and the Early and Periodic Screening, Diagnostic and Treatment (EPSDT) of the Medicaid Act require state Medicaid agencies to provide enrollees under age 21 with access to periodic and preventive screenings, and services that are necessary to “correct or ameliorate” medical conditions, including other additional health care services such as behavioral health conditions. It remains the responsibility of states to determine medical necessity on a case by-case basis. As of 2020, states are mandated to submit a CHIP state plan amendment to demonstrate compliance with the new behavioral health coverage provisions. However, behavioral health services are not a specifically defined category of benefits in federal Medicaid law and coverage of many services is at state discretion. The 2008 Mental Health Parity and Equity Act (MHPAEA) requires that Medicaid managed care and private health insurers who do reimburse for behavioral health services provide behavioral health benefits to cover mental health and substance use services that is no more restrictive than the coverage generally available for medical and surgical benefits. While MHPAEA was designed to reduce inequities in coverage between behavioral and physical health services, it does not reduce inequities in reimbursement as payers are not required to cover behavioral health services.
Ambitious efforts are underway to prioritize behavioral health services for youth. The Department of Health and Human Services (HHS) recently called for states to prioritize and maximize efforts to strengthen youth mental health. The American Academy of Pediatrics (AAP), American Academy of Child and Adolescent Psychiatry (AACAP) and Children’s Hospital Association declared a national emergency in children’s mental health. In addition, passage of the Bipartisan Safer Communities legislation includes significant funding for mental health screening, expansion of community behavioral health center (CCBHC) model; improving access to mental health services for children, youth, and families through the Medicaid program and CHIP; increasing access to mental health services for youth and families in crisis via telehealth; and investments to expand provider training in mental health, supporting suicide prevention, crisis and trauma intervention, and recovery.